The 1918 flu pandemic had a short-lived but devastating effect on Spain, write Sergi Basco (Universitat de Barcelona), Jordi Domènech (Universidad Carlos III) and Joan Roses (LSE). Unlike previous pandemics, it increased inequality, as the better-off could afford to socially distance to protect themselves.
Plagues used to be considered “big levellers”. Death rates were similar across different social groups and reduced income differentials, since the catastrophic mortality increased wages and decreased rents. They also promoted the institutional and technological changes that are behind the economic success of European countries.
Unfortunately, this optimistic interpretation of pandemics fits very poorly with the consequences of the 1918 (Spanish) flu, which is the closest pandemic to COVID-19. Our research on Spain suggests the 1918 flu was not a “big leveller”. Mortality was not equally distributed across different social classes, being higher among the poorest. Spanish flu did not lead to wage increases. And its economic consequences were short-lived, and did not result in institutional reforms and economic development.
Why study the Spanish flu in Spain? Spain is a perfect example of a developing country that was unable to control pandemic mortality in the absence of pharmacological measures and stringent lockdowns. In the early 20th century, Spain was still an agrarian economy. GDP per capita was only 62 per cent of the UK’s in 1918. Manufacturing represented only 27 per cent of total output in 1920, and employed slightly less than 20 per cent of the working population. A large part of the population was poor, by today’s standards, and did not have any savings or property. Education levels were extremely low, and more than half the population was illiterate. Health was appalling, and infant mortality rates were dramatic. Life expectancy was slightly more than 41 years.
Figure 1: Evolution of monthly excess mortality, 1918-20
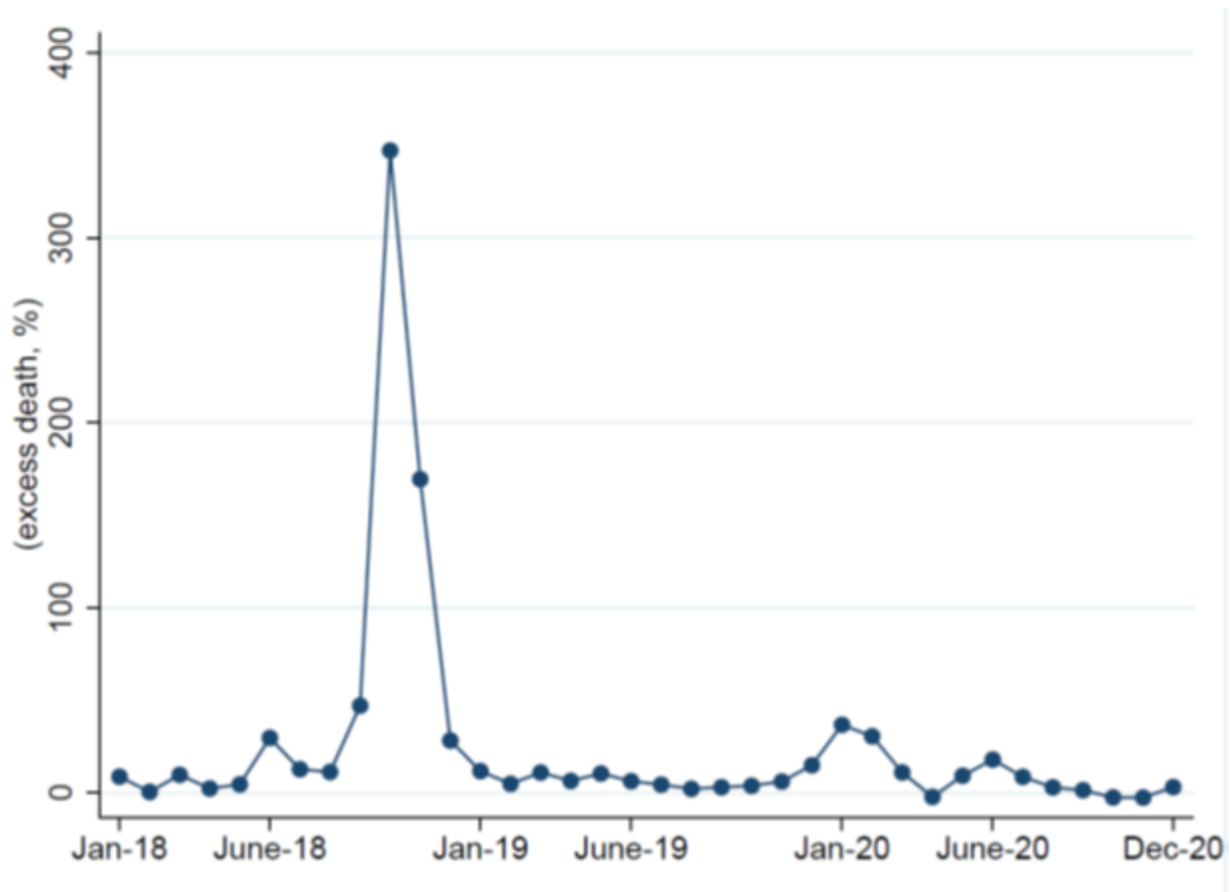
Spanish flu mortality rates were very high—among the highest in the developed world. The flu killed more than a quarter of a million people, about 1.25 per cent of Spanish population. Figure 1 represents the overall series of monthly excess mortality. The data shows the presence of three waves, although the second is several times bigger than the other two. We can observe a small peak in June of 1918. The second wave started in September, reaching a peak in October, and bottoming out in December. Quantitatively, the peak in excess mortality in October is shocking. The number of deaths more than quadrupled those observed in October. There is no sight of the third wave in the winter of 1918/19, although there is a spike in January of 1920. A plausible explanation for the small significant third wave in Spain is that the autumn wave was so intense and the exposure so widespread that Spaniards gained immune protection.

How did the population and authorities react to the flu? Unlike in some other countries, the Spanish population was aware of the spread of the illness. Newspapers regularly published news on the pandemic, and authorities publicised and implemented several measures to fight it. Furthermore, in broad terms, the contemporary scientific understanding of contagion channels was reasonably accurate. Government officials recommended washing hands often and avoiding crowded and poorly ventilated spaces. They cancelled many festivals, local fairs and holidays and closed theatres and music halls. Primary and secondary schools, seminaries, high and technical schools, and universities were also closed. However, there is scarce evidence of mask wearing and none of strict lockdowns and workplace closures. Self-isolation was therefore a personal option, dependent on the availability of sufficient savings. People in isolation had to survive on their own resources, since public support did not exist.
Figure 2: Excess mortality rate by age group in Spain
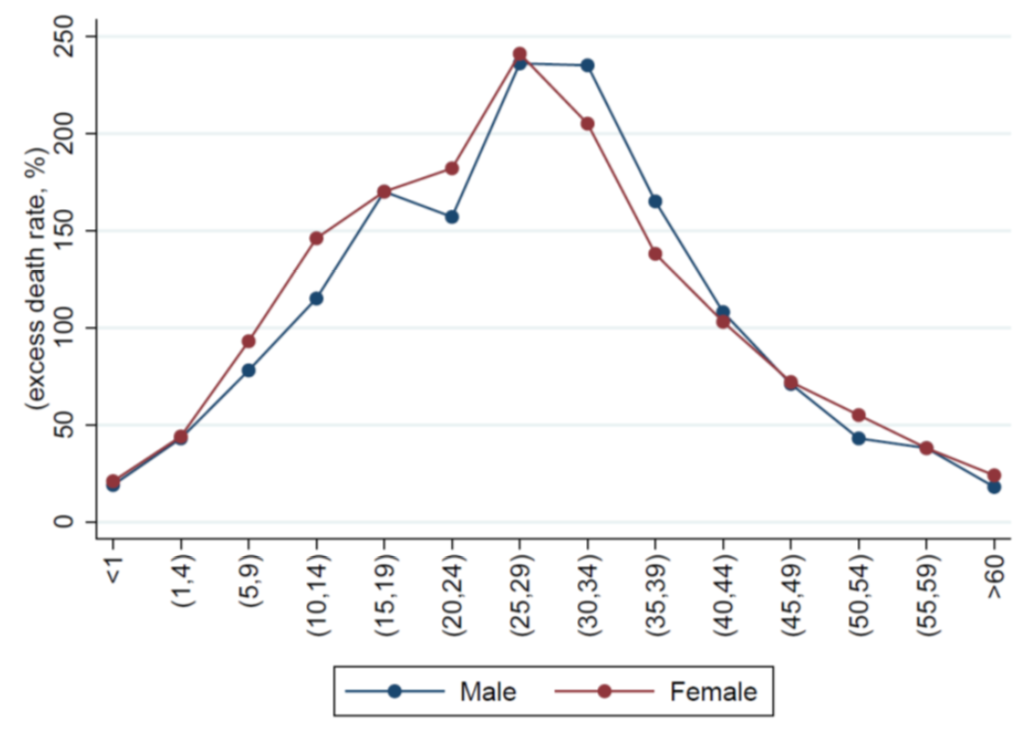
Who died during the Spanish flu pandemic? Unlike with COVID, young adults were the most affected and the peak was in people aged between 25 and 29 (see Figure 2). In addition, the overall excess female mortality rate was 12% higher than the male one. Mortality differentials across regions had a remarkable geographic element related to weather differences. However, the most populous cities were not among the locations most intensely affected by the pandemic.
Were the economic differences important for mortality? The mortality differences among different socio-economic groups are impressive. The high-income group (liberal professions and property owners) had an average excess mortality rate of 29 per cent, compared to 69 per cent in the low-income group and 62 per cent in the mid-income group. Finally, mortality was lower in the most developed regions than in the agrarian ones, and urban mortality was lower than rural. This evidence suggests that mortality differentials were related to the economic capacity of certain social groups to isolate themselves from social contact.
Figure 3: Evolution of Gross Domestic Product and deaths, 1910-1930
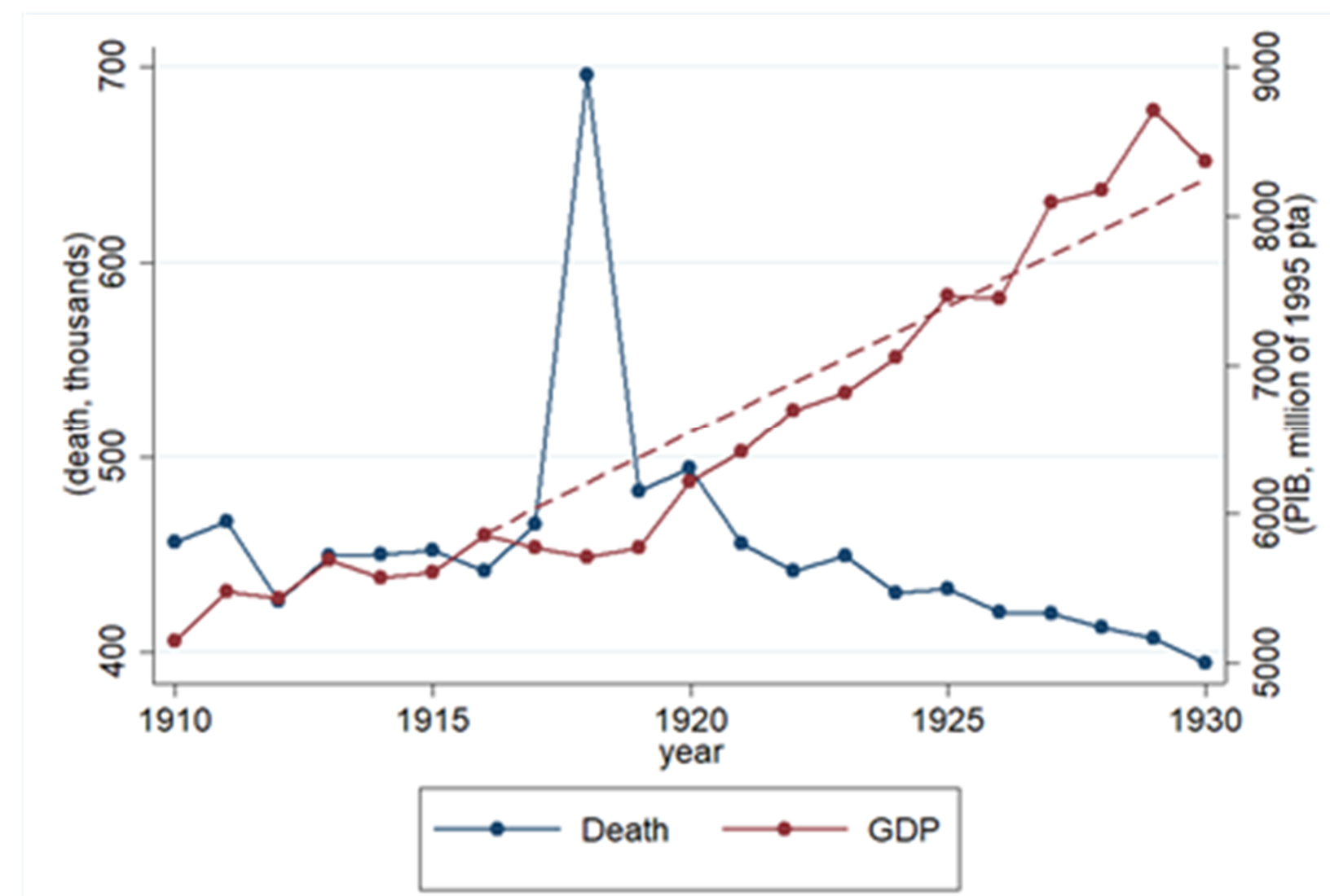
What happened to the Spanish economy? Figure 3 illustrates the evolution of GDP and the sudden increase in the number of deaths in 1918. GDP reached a trough in 1918. Note that even though the decline in aggregate GDP in 1918 does not seem dramatic (only a 1 per cent drop), it represents a substantial deviation from the 1910-1930 trend (6.5 per cent). Most of the decrease is found in services and manufacturing, while the agricultural sector was less affected. Interestingly, harvest was not interrupted due to the pandemic.
Aggregate investment sharply declined in 1918 (by 34.2 per cent), and the fall happened across all investment types. Food consumption slightly increased in 1918, compared to previous years, while demand for non-essential goods significantly decreased (for example, about 20.8 per cent in services). All these shocks were short-lived, since the economy came back in 1919 and rebounded strongly in 1920.
Did Spanish workers benefit from the flu shock? Our research shows large, negative, and broadly short-lived effects of the Spanish flu on real wages. These effects were heterogeneous across occupations. While shoemakers experienced the largest decline in real wages (around 30 per cent), some jobs like metal workers were not significantly affected. In contrast, we fail to find significant negative effects on the returns to capital. Capital gains remained unaffected or positively affected, in the case of house prices, by the pandemic shock. In other words, if anything, the 1918 flu increased inequality.
Our research suggests that the pandemic generated a demand-driven crisis. Mortality was higher in poor and agrarian regions, and real wages decreased more in urbanised and industrialised ones. These negative short-run effects were stronger in occupations in non-essential sectors. The most developed parts of the country experienced a sharp contraction in demand, but avoided the worst death rates.
What are the lessons of the Spanish flu for COVID-19? It led to a decline (delay) in non-essential consumption rather than a fall in production. Although the world economy and the international organisation of production are very different now, the Spanish flu is an example of what could happen in a developing economy in which social distancing is difficult. Social protection and government economic support were scant, the labour market was mainly unregulated, and household savings were scarce. Many people had to work during the worst months of the pandemic and were infected. Without self-isolation, mortality rates were staggering.
This post represents the views of the authors and not those of the COVID-19 blog, nor LSE.



Hey, I am doing an assignment on this precise subject. I cant seem to find authorities speaking about this matter, such as the king or the prime minister, which both were sick with the illness. Do you have any sources where the king or some kind of minister talk about this very evident problem in the country in 1918-19?
You might find this useful: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3867839/