Throughout the world, the share of national income absorbed by healthcare seems to rise inexorably. Technological progress, rising citizen expectations and an ageing population have all helped to propel this escalation in costs. In the United States, almost one dollar in every five is spent on health. In an era of budgetary austerity, policy-makers have been searching desperately for ways to improve the efficiency of healthcare delivery without jeopardising the quality of clinical care. Nowhere is this greater than in hospitals, which are a major component of total healthcare costs.
To an economist, a natural method of improving efficiency is through competition. If patients had more effective, well-informed choice between hospitals, then wouldn’t managers work harder to improve services to attract them?
It is traditionally argued that ‘healthcare is different’ because of multiple market failures. For example, patients typically have poor information about hospital quality and are also unwilling to travel far for healthcare; local doctors are sometimes subject to conflicting incentives; and healthcare is heavily regulated with services often delivered directly by the public sector. Nevertheless, there has recently been a wave of reform in the public services of many countries to create ‘quasi-markets’ and inject greater degrees of patient choice.
In work with Carol Propper and Stephan Seiler, we evaluate whether competition improves hospital quality, in particular by stimulating greater managerial effort. We do this in the context of the acute care hospitals in the NHS.
In the 2000s under the Labour government, resources followed patients and publicly run NHS hospitals had to attract patients to obtain such resources. But since the prices for hospital services were centrally set, the only way hospitals could attract extra patients was by improving quality. Helped by their GPs, patients were given the choice of at least five hospitals and much better information.
Since people dislike travelling far from where they live, hospital competition has a strong geographical element. If competition works, then it should do so more in those areas of the country where there are many hospitals to choose from rather than a single monopoly provider.
There are two major challenges in addressing the question of whether having more hospital competition really improves management. First, how to design ‘an experiment’ that randomly generates more hospitals in some parts of the country than others; and second, how to measure management quality.
The institutional features of the NHS provide a natural experiment for hospital market competition. Entry and exit of hospitals is centrally controlled by the Department of Health and over the last 40 years – and in particular since the mid-1990s – there has been an attempt to reduce the number of hospitals and consolidate services in a smaller number of larger hospitals. Changes in population and demographics are a key consideration in making decisions about how to reconfigure these services.
But politics also matters. Closing down a hospital is highly controversial, as local people will usually fight hard to keep it open. A vivid example of this was in the 2001 General Election when a government minister was overthrown by a politically independent physician, Dr Richard Taylor, who campaigned on the single issue of ‘saving’ the local Kidderminster Hospital, which the government planned to scale down.
We first show what might seem obvious: people blame the central government in power for closing down a hospital and punish them at the ballot box. Hence, it is no surprise that hospitals are rarely closed in constituencies where there is likely to be a close electoral race. For example, the Times reported on 15 September 2006 that ‘A secret meeting has been held by ministers and Labour Party officials to work out ways of closing hospitals without jeopardising key marginal seats.’
Figure 1 shows the number of hospitals in 2005 per head of the population in English constituencies in relation to their political marginality in the 1997 election. There is a surprisingly large number of hospitals in the areas where Labour won or lost with a voting margin of 5% or less. And this relationship holds even after a large number of controls for the area is included, such as income, demographics and population density (the first bar of Figure 2 shows that areas that were marginal had over a standard deviation more hospitals than those that were not marginal).
Figure 1
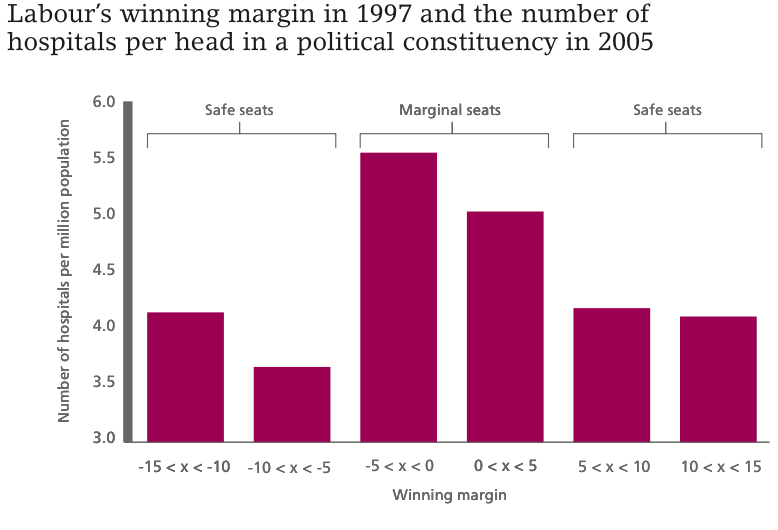
Notes: This figure plots the mean number of hospitals per one million people within a 15km radius of the centre of a political constituency against the ‘winning margin’ in 1997 of the governing party (Labour). When Labour is not the winning party, the margin is the negative of the difference between the winning party (usually Conservative) and Labour. The margin is denoted ‘x’. There are 529 political constituencies in England.
Figure 2
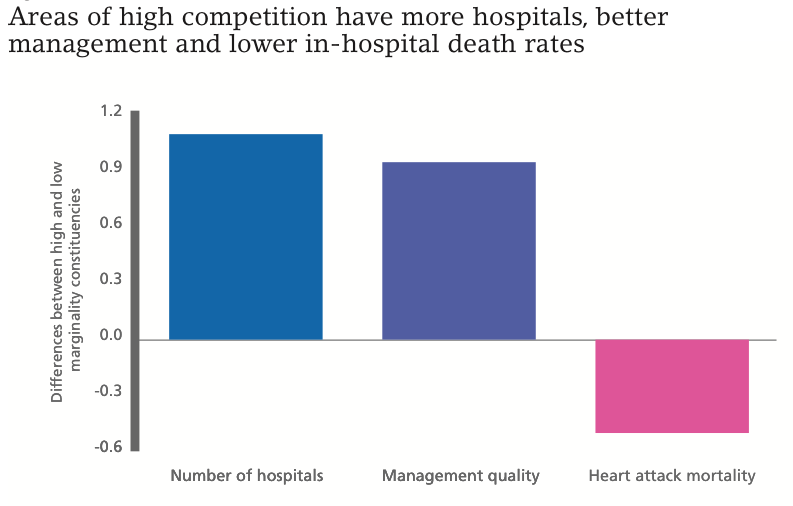
Notes: This figure plots the differences between high and low marginality constituencies (split at the median of marginality after controlling for the baseline regression covariates). All three measures control for many other factors (they are residuals from a regression on these covariates) to strip out the effects of demographics, teaching hospitals, being located in London, etc. The difference between low and high marginality is statistically significant at 1% for the number of hospitals and management quality; and at the 10% level for heart attack mortality rates.
This enables us to use the political marginality of an area as something that for random reasons means that some areas will have more hospitals – and therefore more intense competition – than others. It is a ‘natural experiment’ that gives an additional dose of competition to some areas, which we can compare with others with less competition.
The second question is how to measure hospital management quality. We build on a method for quantifying core aspects of management quality that we first used in 2004 for 732 manufacturing firms in four countries. Since then, the World Management Survey has been expanded to over 20,000 organisations in multiple sectors in 35 countries.
Overall, we find that hospitals that faced more competition had significantly higher management scores and better clinical and financial performance. Using only the random variation in the degree of competition generated by political marginality actually made this relationship between competition and quality stronger. This could be because it is harder to attract good managers to work in areas that are poor and ageing – exactly those areas where health demand and the number of hospitals per head are relatively large.
The magnitude of the competition effect is sizeable. For example, we estimate that adding a rival hospital increases management quality by 0.4 standard deviations and increases survival rates from emergency heart attacks by 8.8%. An illustration of this is in Figure 2: comparing areas that are marginal with those that are not, we find that politically marginal areas had higher management quality (middle bar) and lower death rates (right bar).
We confirm the robustness of our empirical strategy to ‘hidden policies’ that could be used in marginal constituencies to improve hospital management and to changes in capacity that may follow from hospital closure. One concern is that marginality might have direct effects on hospitals through other routes than competition. We show that this is not the case – there is a national funding formula and we confirm that marginality has no effect on financial resources per hospital. Because hospital markets are overlapping, we can even implement a tough test that puts in marginality around a hospital and just uses variation in marginality around its rival hospitals to identify the competition effects. We confirm the absence of such hidden policies associated with political marginality.
Competition can be introduced into public systems by improving information, giving patients and their GPs choice and having money follow the patients. This is a cheaper way of inducing competition than simply building more hospitals, which is expensive. At the moment, decisions over entry and exit of hospitals in public systems usually ignore the effects of competition. Our work suggests that market structure should not be ignored.
The quasi-market in the NHS remains controversial. When our findings on the benefits of competition were first discussed in the media, one of our team members received death threats and had to have security protection when leaving the LSE buildings.
The main objection is that the reforms in the 2000s were thought to be ‘privatising’ the NHS. This is wrong: NHS hospitals are publicly owned hospitals and free at the point of use. Importantly, hospitals are not allowed to compete on price, which is set as a national tariff per treatment type. That leaves quality as the dimension that is open to attract patients. Allowing competition on quality but not price is a safeguard built on experience from the early 1990s ‘internal market,’ when price competition was briefly allowed and led to cuts in costs but also to reductions in quality (which is harder to observe).
Our study also suggests an important role for management. Healthcare is like many other sectors where there is significant scope for improved managerial quality to raise performance. Competition is one way but there are others – improved skills (especially choosing chief executives with some clinical experience) and providing better information are two leading possibilities.
♣♣♣
Notes:
- This article is an excerpt taken from Centrepiece Magazine.
- This post gives the views of the authors, and not the position of LSE Business Review or the London School of Economics.
- Featured image credit: Atlas Genetics test for infectious diseases Matthew Anderson CC-BY-SA-2.0
 Nicholas Bloom is a Professor in the Department of Economics at Stanford University, a Courtesy Professor at Stanford Business School and Stanford Institute for Economic Policy Research, and a co-Director of the Productivity, Innovation and Entrepreneurship Program at the National Bureau of Economic Research. He is a Fellow of the American Academy of Arts and Sciences and The Econometric Society, and the recipient of the Frisch Medal in 2010 and the Bernacer Prize in 2012. His research focuses on the measurement and impact of uncertainty on investment, employment and growth, and the measurement of management practices and productivity.
Nicholas Bloom is a Professor in the Department of Economics at Stanford University, a Courtesy Professor at Stanford Business School and Stanford Institute for Economic Policy Research, and a co-Director of the Productivity, Innovation and Entrepreneurship Program at the National Bureau of Economic Research. He is a Fellow of the American Academy of Arts and Sciences and The Econometric Society, and the recipient of the Frisch Medal in 2010 and the Bernacer Prize in 2012. His research focuses on the measurement and impact of uncertainty on investment, employment and growth, and the measurement of management practices and productivity.
 John Van Reenen is a Professor in the Department of Economics and Director of LSE’s Centre for Economic Performance. He received the European Economic Association’s Yrjö Jahnsson Award In 2009 (jointly with Fabrizio Zilibotti), as the best economist in Europe under the age of 45. In 2011 he was awarded the Arrow Prize for the best paper in the field of health economics. His research focuses on the causes and consequences of innovation, the measurement of management practices and their impact on productivity across firms and countries.
John Van Reenen is a Professor in the Department of Economics and Director of LSE’s Centre for Economic Performance. He received the European Economic Association’s Yrjö Jahnsson Award In 2009 (jointly with Fabrizio Zilibotti), as the best economist in Europe under the age of 45. In 2011 he was awarded the Arrow Prize for the best paper in the field of health economics. His research focuses on the causes and consequences of innovation, the measurement of management practices and their impact on productivity across firms and countries.



