
According to the World Health Organisation, nearly 4 in every 10 dollars spent on health care in the world is spent in the US, a country with only 5 per cent of the world’s population. Even among high-income countries, we know that the US is an outlier, spending almost 18 per cent of its GDP on health, well ahead of the next highest spender, Switzerland, which spends about 12 per cent. There are many different beliefs that have been put forward to explain why the US is such an outlier, relating to the volume and type of services consumed, lack of social spending and prices. Yet new research with my colleagues, Liana Woskie and Ashish Jha, suggests many of these beliefs are incorrect.
Our study brings together a comprehensive set of nearly 100 indicators compiled from a range of international sources. The goal was to examine how well popular explanations for higher spending stand up to the data when we compare the US to ten other high income countries. The data suggest two main factors drive health care spending in the US: higher prices across a wide range of health care services and administrative complexity and costs. This is not a new notion, and reaffirms the finding of late economist Uwe Reinhardt, “it’s the prices, stupid” who made a similar argument in 2003.
What is surprising is that this is the only belief that holds up to the data. Many of the other common beliefs appear to be at odds with the evidence.
Belief 1: The US spends more than other countries because US residents consume much more health care services.
Evidence: on the whole the US is not an outlier in terms of the utilization of health care services. Compared to the other 10 countries, the US has lower rates of physician visits, hospitalisations and days spent in the hospital. The US has average rates of discharges for common conditions such as pneumonia and acute myocardial infarction, and performs more of some surgical procedures (such as knee replacements and caesarean sections) and less of others (such as hip replacements). However, the US does have notably higher utilisation for imaging (MRI and CT scans).
Where data is available, the prices of these services, and pharmaceuticals, appear markedly higher than in the other countries.
Belief 2: The US provides ‘too much’ inpatient hospital care compared to other countries, and does not have enough primary care physicians.
Evidence: The US has among the lowest proportion of health care spending on inpatient services (19 per cent) and among the highest for outpatient services (42 per cent). 43 per cent of US physicians deliver primary care services – the same as the average of other countries.
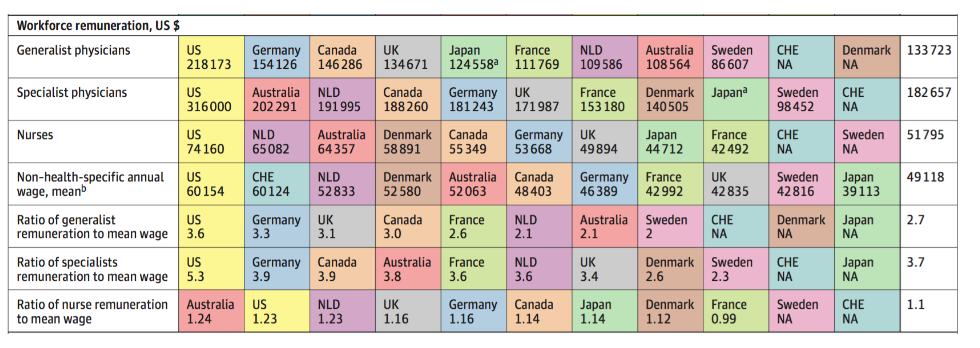
In addition, where data is available, the pay of generalist and specialist physicians and nurses appear markedly higher than in the other countries. The US also pays considerably more on administration costs as compared to other systems, at about 8 per cent of total health care spending (compared to a mean of 3 per cent in other countries). This does not include person-time spent on administrative tasks – where estimates in the US are even higher.
Figure 1 – Remuneration of US health care workforce (click to enlarge)
Belief 3: the US spends more on health care because it spends too little on social services. Therefore the population is sicker and ends up using more care and racking up costs within the health care system
Evidence: Compared to other countries the US has the worst population health outcomes (such as the lowest life expectancy and highest infant mortality). It also has the lowest proportion of the population with health care coverage, 92 per cent.
However, rates of use are similar to other countries. Also, while the US spends less on social services than the mean of the other countries, it still spends more than Canada and Australia and is not an outlier. While low social spending may contribute to poorer population health outcomes, it is unlikely a primary driver of higher health care spending.
Belief 4: the quality of care is lower in the US generating waste and inefficiencies
Evidence: Despite having the worst population health outcomes, the US has the best outcomes for patients who suffer from an acute MI or stroke, and is average to below average for avoidable hospitalizations of patients with diabetes and asthma.
So where do we stand? Our findings suggest that if the US wants to learn lessons from other high-income countries, we must ensure they are the right ones. We cannot cherry pick based on our preconceptions; nor can we look at drivers in isolation. With this comprehensive perspective it becomes clear that, moving forward, focus must be on the high price of health care services and finding ways to lower those prices while maintaining or even improving the quality of care.
♣♣♣
Notes:
- This blog post appeared originally on LSE USAPP. It is based on the paper Health Care Spending in the United States and Other High-Income Countries, in the Journal of the American Medical Association.
- The post gives the views of its authors, not the position of LSE Business Review or the London School of Economics.
- Featured image credit: Photo by sasint, under a CC0 licence
- When you leave a comment, you’re agreeing to our Comment Policy.
 Irene Papanicolas is an Assistant Professor of Health Economics in the Department of Health Policy at the London School of Economics and a Visiting Assistant Professor at the Department of Health Policy and Management at the T.H. Chan Harvard School of Public Health. Her research focuses on performance measurement of health systems and health services.
Irene Papanicolas is an Assistant Professor of Health Economics in the Department of Health Policy at the London School of Economics and a Visiting Assistant Professor at the Department of Health Policy and Management at the T.H. Chan Harvard School of Public Health. Her research focuses on performance measurement of health systems and health services.



