Vaccines are protective interventions that can have a long-lasting impact on our health. Although in public minds vaccines are associated with diseases that were thought to be eradicated in many western countries, COVID-19 has brought them back to the spotlight. What defines vaccines is that they are provided to healthy individuals, hence their value lies in their ‘preventive or protective effect’, and in getting enough people to get vaccinated so as to give rise to herd immunity. However, vaccine availability does not necessarily entail widespread vaccination. A share of the population in almost all societies refuses to get vaccinated. Hence, actual vaccination is not just the result of access, but the acceptability of specific vaccines. It’s important to understand those who refuse to get vaccinated, and how to change their minds.
Most people will get vaccinated, but far from everyone,….
A recent global survey suggests that 71.5% of people are likely to take a COVID-19 vaccine, and 61.4% would accept their employer’s recommendation to do so. However, a recently released IPSOS survey below finds a large variation across countries, with 80% of people in China intending to take the vaccine and half that figure (40%) in France and Russia. In almost all countries, the proportion of individuals who say they will get vaccinated dropped from October to December.
Figure 1. If a vaccine for COVID-19 were available, I would get it
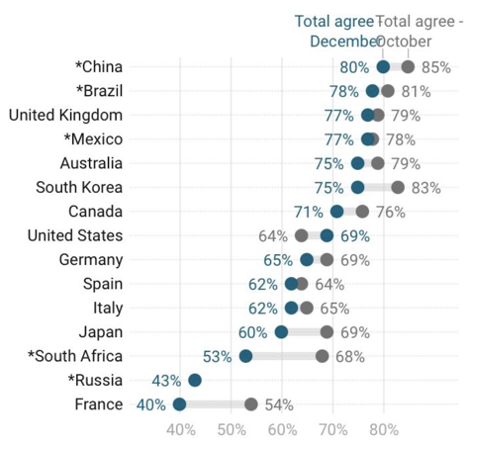
Source: IPSOS, 2020
Why do people refuse to get vaccinated?
The main concern is that people lack proper knowledge of how vaccines benefit them, or they feel they should be able to control the potential side effects. Limited knowledge might make some individuals vulnerable to fake news, or lead them to overestimate some rare side effects and focus on the loss these side effects would entail, as opposed to their low probability of occurrence. As a result, availability of information on side effects, alongside limited knowledge, feed what can be defined as ambivalent preferences, which the vaccine-specific literature defines as ‘vaccine hesitancy’. Furthermore, less educated, less pro-social and more risk-averse individuals are less likely to get vaccinated.
In 2019 the WHO identified vaccine hesitancy as one of the top ten global health threats, which they define as the ‘delay in acceptance or refusal of vaccination despite availability of vaccination services’. Although individuals are aware of the existence of a vaccine, the information available in their choice architecture does not suffice for them to come to a definitive decision. This is not unique of vaccines. We find similar ambivalence when we look at attitudes to GM foods, as individuals do not fully understand what they are being offered.
One of the main drives of vaccine hesitancy is the underestimation of vaccine safety, and more specifically the increasing awareness of potential side effects, which seems to have a large impact on public perceptions. Similarly, individuals who underestimate the COVID-19 risks are less likely to get the vaccine, as they might not perceive the virus as an imminent threat, or might downplay it (e.g., COVID-19 is often compared to the influenza, or it is said to be a risk for older-age individuals only). A survey of Australian attitudes to COVID-19 suggests that almost half (44%) of those who said they would not get the vaccine were more likely to believe the threat of COVID-19 had been exaggerated.
The other main pushback that bolsters vaccine hesitancy is distrust in health authorities, and the medical profession more generally. Knowledge about vaccines is generally limited both between individuals who take them as well as those that refuse them, and when knowledge in limited individuals tend to rely on trust. Some evidence suggests that trust in the medical profession is a central issue in children vaccination decisions. As a matter of fact, the waning trust in vaccines has been a cause of concern that led to the set-up of the World Health Organization’s SAGE, Strategic Advisory Group of Experts on Immunisation worldwide. Weak trust is especially concerning now that we depend so badly on the uptake of a vaccine to get over the COVID-19 pandemic.
So, what can governments do?
- Subsidies and payments: One way to go is to subsidise vaccine uptake among those individuals that are more likely to be vaccine-hesitant. However, this might entail some significant costs and possibly might require strategic decisions. Furthermore, some evidence suggest that paying people to get vaccinated might signal risk, and backfire as a strategy.
- Compulsion: vaccination can be made compulsory given the spillover effects on others, especially older-age individuals. However, the administrative costs to operationalise compulsory vaccination might be counterproductive as they can feed further antagonism and resistance.
- Nudges: both positive and negative nudges can be considered above and beyond other policies influencing reference points and vaccination framing. Changing the narratives of vaccination so individuals that refuse to vaccinate understand that the default option is to vaccinate can make a difference. The role of celebrities taking up vaccines and promoting them is important. Experimental research points to social nudges that reward vaccination, portraying it as a pro-social behaviour.
- Conditioning: conditioning access to certain entertainment activities or visits to publicly funded medical services or schools to having been vaccinated, or marginally changing cost-sharing for those individuals that refuse to vaccinate. Positive incentives might include the conditioning of receiving benefits to being vaccinated, among others.
- Social incentives (esteem, stigma): naming and shaming individuals that refuse to vaccinate can be an effective cognitive cost to someone’s reputation as a ‘good citizen’. Spain has developed a list of individuals who have refused to be vaccinated. A register will include all the people who turned down the vaccine after being called up for vaccination by Spain’s public health service. Some ‘vaccine-hesitant ‘individuals might decide to take up the vaccine if that takes them off the list.
- Rising risk awareness: rather than hiding the deaths from COVID-19, there is an important role for the media to portray an accurate representation of the people dying from COVID-19. Risk and benefit perceptions are interrelated as we suggest in our research. If individuals do not perceive the risks, they are unlikely to see the benefit of taking up the vaccine.
- Trust building strategies require the mobilisation of key stakeholders such as community and local leaders or trade unions to support public health authorities and the medical profession to confront the credibility of anti-vax sources. For instance, general practitioners (GP) have a key role to play. Evidence from France, the country which exhibits the lowest vaccination intentions as presented above, suggests that a significant share of GPs consulted vaccine-critical information sources and might not have pushed vaccination as much as they could.
So, what does it mean?
Countries should put together a strategy sooner rather than later. The core of the vaccination question lies on trust building, raising awareness as well as putting forward nudging and conditioning strategies that change people’s narratives, where the default is that vaccination is the straightest route to the progressive return to a life that compared to the one before the pandemic.
♣♣♣
Notes:
- This blog post expresses the views of its author(s), not the position of LSE Business Review or the London School of Economics.
- Featured image by Daniel Schludi on Unsplash
- When you leave a comment, you’re agreeing to our Comment Policy
 Joan Costa-Font is an associate professor (reader) at LSE’s department of health policy. He is an economist affiliated with CESIfo in Munich and IZA, Bonn. The core of his current research focuses on health and behavioural economics.
Joan Costa-Font is an associate professor (reader) at LSE’s department of health policy. He is an economist affiliated with CESIfo in Munich and IZA, Bonn. The core of his current research focuses on health and behavioural economics.



I am, regrettably, one of those who are reluctant to take the vaccine. At 76 I should be welcoming it but I am doubtful about the speed that this vaccine has been developed compared with, say, the flu vaccine. I also recall reading an article by a Dr Michael Yeadon who said there was no need to vaccinate healthy people.
Good afternoon,
I am afraid ,after listening to anna Rothschild delivering a Q+A session with Dr Margaret Liu where ms rothschilled
sniggered her way through ‘a chefs ingredient list’ only to point out later that there is another ingredient that is NOT on the chefs list ‘polyethylene glycol PEG, no thank you.
There can be no errors, one vaccine does not fit all, and anna rothschilled should observer that every person dying/reacting badly to any vaccine is someones relative, so perhaps someone professional should be delivering these podcasts because frankly she was reading from a queue.
About the vaccine itself ,I will wait , like the best of them, until everyone else has had their shot then perhaps I might think about it.
Kind Regards
Eilis Woods
A culture of ‘naming and shaming’ would most certainly provoke resistance amongst many. Some in society (granted a minority) have no interest in having accord with the group consensus. Further, many of the proposed strategies compiled here are psychologically exploitative and therefore ethically questionable. Trust and intelligent debate allied to worthy example are the only authentic means of approaching this issue. But then we know if push comes to shove, which is likely, then such measures will most certainly be employed.
I will not accept any vaccine , as a child I had no choice, now I do. Why? Well its purely my inherent distrust of a sudden panacea that seems to good to be true. Time will tell- and I’m sure I will be proved wrong in due course?