The widespread malnutrition of children in South Asia is persistent and troubling. Given the importance of religion in the region, Elizabeth Brainerd and Nidhiya Menon examine the relationship between inequalities in child health and religious identity across India, Bangladesh and Nepal. They find a consistent trend of Muslim advantage in infancy, vis-à-vis Hindus, and its reversal after 12 months of age across the three countries.
The widespread malnutrition of children in South Asia is persistent and troubling. Given the importance of religion in the region, Elizabeth Brainerd and Nidhiya Menon examine the relationship between inequalities in child health and religious identity across India, Bangladesh and Nepal. They find a consistent trend of Muslim advantage in infancy, vis-à-vis Hindus, and its reversal after 12 months of age across the three countries.
Children in South Asia are among the most undernourished in the world. In Bangladesh and Nepal, for example, over half of the children under five years of age suffer from chronic malnutrition (low weight-for-age). In India, nearly 48% of all children were stunted (low height-for-age) in 2007 according to World Bank data (World Development Indicators, 2012). The rates of stunting and undernourishment in all three countries are higher than in many countries of sub-Saharan Africa with lower levels of per capita income and higher rates of infant and child mortality (Deaton and Drѐze 2009, Jayachandran and Pande 2014). There is some evidence, albeit inconsistent, that this trend has continued during the 1990s and early 2000s (Deaton and Drѐze 2009), a period of time when both India and Bangladesh experienced significant economic growth and made rapid progress in reducing poverty. Even among affluent Indian households, a substantial proportion of children are undernourished by most anthropometric indicators (Deaton and Drѐze 2009). Our research investigates the puzzle of child undernourishment in India, Bangladesh and Nepal by comparing differences in child health outcomes by religious affiliation (Brainerd and Menon 2015).
Analysing inequalities in child health by religious identity
Religion plays an important role in these countries. India and Nepal are Hindu majority countries whereas Bangladesh has a Muslim majority. The religious affiliation of a child’s family provides information on the likely dietary restrictions1 encountered by a child in his or her early growing years, on the child’s exposure to fasting in the womb during the Muslim holy month of Ramadan, and on possible differences in women’s autonomy and control over household resources arising from differences in son preference across religions (Jayachandran and Pande 2014, Coffey et al. 2013). All of these are factors that may contribute to the high rate of stunting and wasting among the children in these countries. Since one is born into one’s religious identity and marriage is often restricted to one’s caste and faith in these regions, these three countries provide an especially pertinent context in which to analyse the causes of inequality in child health status by religious identity.
We focus on children from birth to five years of age. The health of children at these young ages is critically important, as a wealth of recent evidence demonstrates that negative health shocks in this period can have large, long-lasting effects extending well into adulthood (see, for example, Currie and Vogl 2013). While most of this literature has focused on children in the developed world, children in developing countries are likely to be even more vulnerable given the prevalence of insults to health (nutritional, environmental and toxic) and widespread adherence to behaviour that may have harmful effects on children’s health, such as fasting during pregnancy. Negative health shocks to children in developing countries have only recently begun to receive attention in the economics literature (Almond and Mazumder 2011, Brainerd and Menon 2014).

Our study uses a number of datasets to assess inequalities in child health by religion. Our main analysis uses several recent rounds of the Demographic and Health Surveys (DHS) for India, Bangladesh and Nepal to examine differences in child anthropometric measures by religion, age and gender within each country. The DHS surveys provide a rich source of data on child, mother, and father characteristics, including detailed fertility histories of women aged 15 to 49. The period we analyse is approximately 1999–2011 (depending on the country), a time span in which all three countries experienced strong economic growth and declining poverty rates.
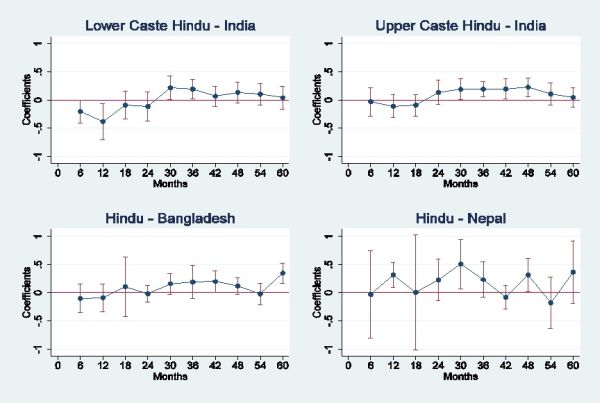
Our results indicate that Muslim infants (age less than 12 months) have a significant advantage in height-for-age and weight-for-age z-scores2 over low-caste Hindu infants in India. In Bangladesh, Muslim male infants have better height-for-age as compared to Hindu male infants, and Muslim female infants have better weight-for-age than Hindu female infants3. However, this advantage does not persist past infancy; looking at the one to five years age group, Hindu children (upper-caste Hindus in India) are significantly taller and heavier than Muslim children in all three countries. Two additional datasets for South Asian children confirm these patterns (Young Lives Survey and the 2004 Health Survey for England). These datasets sets allow us to rule out mortality selection (weakest infants die and so the samples of older children have a larger proportion of strong children than should be the case in samples that are representative) as a cause of the reversal, and further suggest that the early Muslim advantage is likely to be cultural – and possibly linked to religious practices (hand-washing before prayers) – rather than country-specific. Figure 1 below provides a graphical depiction of our results.
The puzzle of Muslim health advantage in infancy and its later reversal
While a Muslim advantage in child survival in India is well-known (Bhalotra et al. 2010), the pattern of Muslim advantage in infancy, its reversal after 12 months to a Muslim disadvantage, and its consistency across these three countries has (to the best of our knowledge) not been previously documented. As we demonstrate, the reversal in Muslim health advantage is not explained by static differences in family background or living conditions between Muslim and Hindu children (such as mother’s education, mother’s height, age at marriage, access to sanitary facilities, or household assets), nor is it explained by differences in child characteristics such as birth order, breastfeeding, prenatal care, or disease incidence. The Muslim advantage in height for male infants is especially surprising for India, in which the preferential treatment of boys (thought to be greater among Hindus) begins even in the womb (Bharadwaj and Lakdawala 2012) and extends after-birth to lengthier breastfeeding and greater vitamin supplementation (Jayachandran and Kuziemko 2011, Barcellos et al. 2014). We test for possible explanations for the reversal of the Muslim health advantage and find that for boys in India, the most likely explanation is the observance of fasting during Ramadan by Muslim women, which appears to lead to a ‘positive selection’ of male infants4 but still has long-lasting negative health effects on all surviving Muslim children. However this does not explain the patterns among girls, nor does it explain the reversal of the health advantage for Muslim infants in Bangladesh. In this sense, the Muslim health advantage in infancy and its later reversal in these three countries remain a puzzle.
Concluding remarks
The widespread malnutrition of children in South Asia is persistent, troubling, and poorly understood. Given that religion dictates many of the rituals of daily life for much of this population – from dietary restrictions and fasting, to hand-washing and daily prayer – our paper investigates differences in child health by religion to better understand the high rates of stunting and wasting among children in these countries. The detailed data and comparative research design we use allows us to account for many socioeconomic characteristics of children and families, and to establish that remarkably similar patterns of child malnutrition by religious affiliation occur across all three countries we study. The reversal in Muslim advantage in infancy to Hindu advantage among older children, even in Bangladesh, a country with a Muslim majority, is a puzzle. In addition to the positive selection of Muslim (male) infants, it is also possible that differences in hygienic practices, such as hand-washing before daily prayer among Muslims, explain the Muslim health advantage in infancy. We are not able to investigate this possibility, although hygiene differences would have to be more important for infants than for young children for this to explain the patterns we observe. A future line of research would explore other Muslim-Hindu differences in cultural practices, in infant and child care, or in intra-household allocation of resources to women and children which we are unable to observe in our data but may explain the Muslim-Hindu differences in child health outcomes we document.
- For example, upper-caste Hindu children will not consume any form of meat or eggs and will switch to consumption of rice away from breast milk relatively quickly. Son preference is believed to be stronger among Hindus and women’s autonomy, especially of the youngest daughters-in-law, is believed to be the weakest.
- The indicators are measured in terms of z-scores which capture how much a child’s weight/ height deviates from that of an international reference group of healthy children of the same age who are raised in a healthy environment, as proposed by the World Health Organization (WHO) (2006).
- In our analysis for Bangladesh, Hindus are not differentiated by caste status as we lack that data.
- Male foetuses are more susceptible to shocks and so the weaker ones die; this means that male infants who are born are relatively more ‘strong’ (positive selection).
This article was originally posted on Ideas for India 3 July 2015.
Note: This article gives the views of the author, and not the position of the South Asia @ LSE blog, nor of the London School of Economics. Please read our comments policy before posting.
About the Authors
Elizabeth Brainerd is the Susan and Barton Winokur Professor in Economics and Women’s and Gender Studies at Brandeis University.
Nidhiya Menon teaches courses in development economics and statistics. She has been a researcher at the Grameen Bank in Bangladesh, and a consultant with the Development Economics Research Group and the Economics and Development Institute of the World Bank.