More six percent of U.S. children regularly take stimulant medication, often in order to help them manage in school. But what factors shape stimulant use amongst adolescents at school? In new research which analyses prescriptions for stimulants in the U.S., Marissa King finds that economically advantaged children are more likely to use stimulants in response to academic pressures, and that states with stricter school accountability policies for pupil performance see greater stimulant use amongst children. Making schools more academic, she writes, appears to encourage school-based stimulant use.
More six percent of U.S. children regularly take stimulant medication, often in order to help them manage in school. But what factors shape stimulant use amongst adolescents at school? In new research which analyses prescriptions for stimulants in the U.S., Marissa King finds that economically advantaged children are more likely to use stimulants in response to academic pressures, and that states with stricter school accountability policies for pupil performance see greater stimulant use amongst children. Making schools more academic, she writes, appears to encourage school-based stimulant use.
Stimulant medications, which improve concentration and help manage other symptoms associated with attention-deficit hyperactivity disorder, are the most widely used class of medications among adolescents in the United States. Roughly 6 percent of children in the US take a stimulant medication such as Ritalin or Adderall. Over the past two decades, stimulant use in the United States has more than doubled. Despite this dramatic rise, how factors such as family and schooling shape patterns of stimulant use remain poorly understood. In new research, we find that schooling is a strong driver of stimulant prescriptions. Moreover, economically advantaged children were more likely than their less advantaged peers to selectively use stimulants in response to academic pressure.
Children and adolescents are considerably more likely to take prescription stimulants during the school year than during the summer, a behavior we dub “school-based selective stimulant use.” Prescription fills among school-aged stimulant users increases by 30 percent during the school year.
To better understand school-based selective stimulant use, we analyzed a dataset that includes the majority of stimulant prescriptions written in the United States. As Figure 1 shows, in a given week during the school year roughly 17 percent of adolescent stimulant users filled a prescription. Put differently, this means that the average family filled a prescription every 41 or 42 days. This is approximately what we would expect to see if children were taking stimulants during the school week but were taking drug holidays on weekends. Stimulant prescription fills drop considerably in the summer. Differences in school year and summer use could not be explained by medication side effects, medication cost, or type of attention deficit hyperactivity disorder (ADHD).
Figure 1 – Adolescent use of stimulants during the school year by socioeconomic group
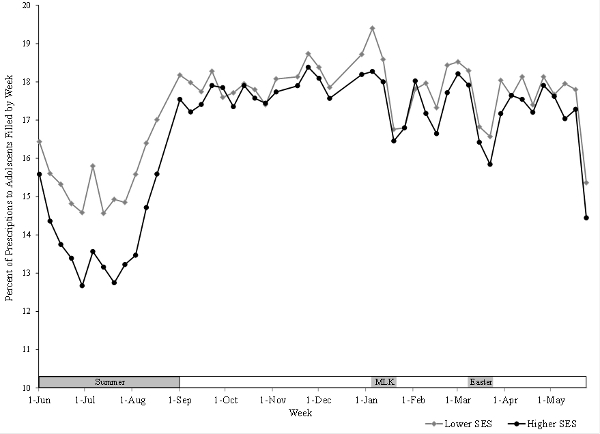
Children and adolescents from socioeconomically advantaged families (shown in black) were more likely than their less advantaged peers (shown in grey) to selectively use stimulants during the school year. There are at least two possible explanations for the differences we observe among adolescents of higher and lower socioeconomic status (SES). On the one hand, higher-SES children may see doctors whose beliefs about how stimulants should be used differ from the practice styles of doctors typically seen by lower-SES children. Alternatively, higher-SES families might be more likely to selectively use stimulants in order to meet the behavioral and academic demands of schools. We compared higher and lower socioeconomic status children who were seeing the same doctor to adjudicate between these possibilities. Socioeconomic differences in school-based selective stimulant use persisted among children seeing the same doctor. This suggests that parent preferences, not physician practice styles, explain higher rates of school-based selective stimulant use among economically advantaged children.
To examine the importance of academic pressure in shaping patterns of selective stimulant use, we exploited differences in the rigor of states’ educational accountability policies. States have implemented accountability policies that often punish or reward schools for student performance on standardized tests in an attempt to hold them accountable for student achievement. Schools have become increasingly academic in response to accountability policies. Time devoted to test preparation and math instruction time has increased, while the time allotted for recess, art, and physical education has decreased. In school environments with relatively strict accountability policies where academic pressure is intense, we anticipated that selective stimulant use would be more common.
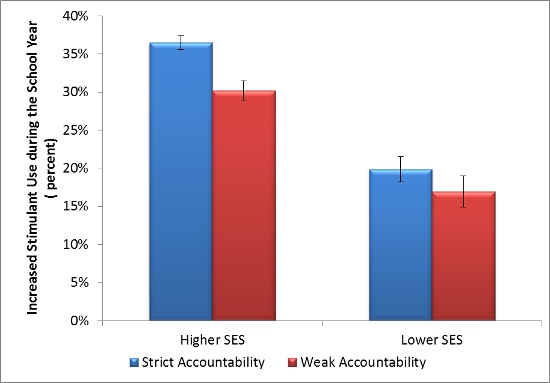
School-based selective stimulant use occurs most frequently in states with strict accountability policies among economically advantaged children. Figure 2 shows selective stimulant use in states with strict and weak accountability policies. We used state rankings of school accountability policies published by Education Week which grades states based on the extent to which they have adopted clear and specific academic standards, how well state standards align with state tests, and the degree to which the state holds schools accountable for their performance to classify states as either strict accountability or weak accountability regimes. There is considerable state-to-state variability in the stringency of accountability policies. Strict accountability states are shown in blue and weak accountability states are shown in red. In states with weak accountability policies, there was not a significant difference in selective stimulant use by socioeconomic status. In states where academic pressure is intense, selective stimulant use increases, especially among economically advantaged children. Thus, selective stimulant use may offer a new pathway through which medical interventions allow higher SES families to reproduce academic inequality, either purposefully or inadvertently, since stimulants have been shown to aid in concentration and attention.
Figure 2 – Stimulant use by adolescents in states with strict and weak accountability policies
To be clear, we do not believe that students or their families are selectively using stimulants to aid in test performance. Rather we believe that accountability policies create schooling environments in which parents and children find it necessary to take stimulant medication to manage intense academic pressure and attentional demands. More economically advantaged families appear to more frequently meet these demands through selective stimulant use.
For decades, parents have often faced a difficult question: Do they medicate their child to help them manage the attentional and behavioral requirements of school? As a society, we now stand at a similar juncture. Making schools more academic appears to encourage school-based selective stimulant use. Rather than medicating children to help them manage the increasing attentional demands of schooling, perhaps it makes sense to offer more recess and focus just a little less on standardized tests?
This article is based on the paper, ‘Medical Adaptation to Academic Pressure: Schooling, Stimulant Use, and Socioeconomic Status’, in the American Sociological Review.
Featured image credit: ep_jhu (Flickr, CC-BY-NC-ND-2.0)
Please read our comments policy before commenting.
Note: This article gives the views of the author, and not the position of U.S.App– American Politics and Policy, nor of the London School of Economics.
Shortened URL for this post: http://bit.ly/1CcQTzg
_________________________________
Marissa King – Yale University
Marissa King is an Assistant Professor in the Yale School of Management with a secondary appointment in Sociology. Professor King’s current research examines patterns of antidepressant, stimulant, and antipsychotic utilization. In general, her research analyzes the spatial and temporal dimensions of innovation and diffusion.