Individuals increasingly rely on healthcare virtual support communities (HVSCs) to complement and/or supplement the support available in face-to-face settings. Many reasons contribute to this phenomenon. While relatives and close friends can provide physical and tangible assistance (providing goods or services needed during stressful situations), these helpers oftentimes lack stress- or disease-related expertise and experience to provide adequate support. Additionally, patients may be inhibited by communication impairment or mobility issues, or feel reluctant to burden close social networks, or fear stigmatisation due to the illness.
Joining HVSCs allows individuals to interact anonymously without social stigmatisation. Participants usually get access to more support (because of the size of the network) or better quality (because of easy access to greater expertise from people with similar experience). Further, it is also easier to obtain support when it is most needed (oftentimes in the middle of the night when anxiety tends to be higher). Through the sharing of personal feelings and emotions, coping stories, and life events, people learn from each other’s experiences, and develop strong relationships, attachments, and norms of how to render help.
While researchers know a lot about the reasons why individuals join these communities and how they affect health outcomes, we know very little about the factors that drive members of HVSCs to voluntarily help and support others. This is a fundamental issue since the success of HVSCs in helping and connecting support seekers depends on the willingness of community members to voluntarily contribute.
Discovering the success factors will also help virtual support community designers and healthcare organisations create a community conducive to social support exchange. In our recent paper, we studied online cancer support discussion forums hosted by the American Cancer Society’s Cancer Survivors Network (CSN) to explore this research question. The CSN hosts discussion forums for various kinds of cancers and the three most active discussion forums of this community – colorectal cancer, breast cancer, and prostate cancer discussion forums – were chosen as the data source from which more than 32,000 discussion messages, contained in 2,537 threads, were collected.
We first applied machine-learning approaches to automatically classify online messages into the following three voluntary helping behaviours.
Informational support
Support that reduces uncertainty and/or facilitates problem-solving. E.g., a support provider shared his/her personal experience about two medications: “I was first put on Femara. However, I had to switch to Tamoxifen as I could not tolerate the side effects of the Femara….”
Emotional support
Support that restores emotional stability through the communication of love, sympathy, empathy, and encouragement. E.g., one forum member posted a message to remind another member of the availability of supportive others: “We have to be glad for the prayer warriors out there … they never stop praying for any of us. You and I and many like us have to remember that. Someone is praying now.”
Companionship activities
Camaraderie, joking, and sharing entertaining stories. E.g., on a community member’s birthday, one member posted: “Today is Gogers’ Birthday! Hoping your day is filled with wonderful surprises and love all around you!”
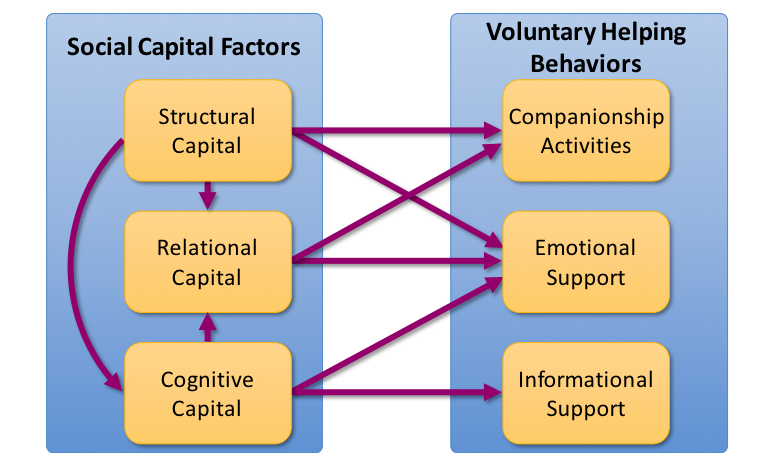
Drawing on social capital theory, we subsequently analysed the social capital components that were manifested in online message content. That included structural capital (social interaction frequency, intensity, and multiplexity that represent social connections between online participants), relational capital (relationship qualities such as trust, social norms, and common identity) and cognitive capital (resources such as shared language and healthcare experience that promote mutual understanding and interpretations). We wanted to see how online social capital drives different voluntary helping behaviours in HVSCs.
We found that while all three aspects of social capital were positively associated with voluntary provisions of emotional support, only cognitive capital directly predicted online contributions of informational support. Structural capital, while having no direct effect on the voluntary provisions of informational support, indirectly affected informational support via cognitive capital. We also found that structural capital and relational capital are positively associated with individual participation in companionship activities. Additionally, through relational capital, structural capital and cognitive capital indirectly affected emotional support and companionship activities. Figure 1 illustrates the findings of our study.
The importance of building structural capital
Our findings on the direct and indirect effects of structural capital suggest that, as HVSCs consist primarily of lay people with little professional healthcare-related expertise, it is crucial to encourage members to engage in intense, frequent, and multiplex interactions with other members. This can be achieved by creating visually appealing and well organised content with clear navigation paths, having community experts update content regularly, and developing community tutorials, video introductions, and FAQ sections. Additionally, inviting healthcare professionals to participate and share useful information, and making it easier for members to locate experts in the community will help address the urgent needs of community members and foster interactions. Creating a reputation mechanism that identifies top contributors can also encourage member participation.
The importance of increasing relational capital
Social identity, trust, and helping norms (relational capital) in HVSCs promote emotional support provision and encourage companionship activities. Since participating requires extensive disclosure of personal, sensitive information, community designers and administrators need to assure members about the safety of sharing such personal information. Clear policies highlighting the security of shared information and membership anonymity, and a welcome message showing the clear purpose of the community, intended audience, and information about site managers will increase trust among community members. Welcome or “sticky” messages (the ones that are pinned on the top of the message board) highlighting and reminding members of the similarities among community members and the importance of being “answer people” for others facing stressful situations will also promote community identification and helping norms.
The importance of increasing cognitive capital
Cognitive capital is the sole source of informational support provision in HVSCs. It is therefore essential to equip community members with healthcare-related expertise. Non-familiarity with the terminology and rituals used in virtual communities and a perceived lack of required knowledge to participate can contribute to community members’ “lurking” behaviour. The direct relationship between structural capital and cognitive capital suggests that facilitated member interactions will lead to the acquisition and development of shared language and healthcare-related expertise. The introduction of experts to a community, together with a community design allowing community members to identify these experts, and regular education webinars can stimulate discussion among community members and community experts and encourage knowledge acquisition and creation.
The importance of tailored interventions
Different types of social support and companionship activities may be influenced by different social capital components, as shown in Figure 1. Healthcare practitioners can design appropriate interventions to foster the provision of the type of support that is more effective and preferable in a given HVSC. For example, healthcare organisations seeking to enhance the quality of their offerings by tapping into patients’ knowledge and experience would prefer informational support in HVSCs. Cognitive capital development among members of this community type will help achieve the goal. Additionally, the offering of emotional support could be stressed by HVSCs intended for individuals with low levels of control over the stressors and diseases (optimal matching theory), such as cancer and mental disorders. This can be done through the development of structural capital and relational capital in HVSCs.
♣♣♣
Notes:
- This blog post is based on the authors’ paper Sharing Is Caring: Social Support Provision and Companionship Activities in Healthcare Virtual Support Communities, MIS Quarterly (forthcoming)
- The post gives the views of its authors, not the position of the institutions they represent, LSE Business Review or the London School of Economics.
- Featured image credit: Photo by kropekk_pl, under a CC0 licence
- When you leave a comment, you’re agreeing to our Comment Policy.
 Kuang-Yuan Huang is a faculty member of Computer Information Systems in the Hasan School of Business at Colorado State University – Pueblo. His research interests are centred around the behavioral and social aspects of information systems use, specifically social uses of virtual communities and social media, technology supported knowledge management, technology adoption, and healthcare information technologies. His research has appeared in top academic journals.
Kuang-Yuan Huang is a faculty member of Computer Information Systems in the Hasan School of Business at Colorado State University – Pueblo. His research interests are centred around the behavioral and social aspects of information systems use, specifically social uses of virtual communities and social media, technology supported knowledge management, technology adoption, and healthcare information technologies. His research has appeared in top academic journals.
 InduShobha Chengalur-Smith is a faculty member in the Information Systems & Business Analytics department at the School of Business in the University at Albany, SUNY. She received her Ph.D. from Virginia Tech and prior to joining academia she worked in both the private and the public sectors. Her research interests are in the areas of Virtual Communities, Technology Adoption and Implementation, and Information Quality and Security. She has worked on federally sponsored grants as well as industry-sponsored projects, ranging from best practices in computational thinking to technology implementation. She serves on the editorial boards of Information & Management and the ACM Journal of Data and Information Quality and her research has been published in leading academic journals.
InduShobha Chengalur-Smith is a faculty member in the Information Systems & Business Analytics department at the School of Business in the University at Albany, SUNY. She received her Ph.D. from Virginia Tech and prior to joining academia she worked in both the private and the public sectors. Her research interests are in the areas of Virtual Communities, Technology Adoption and Implementation, and Information Quality and Security. She has worked on federally sponsored grants as well as industry-sponsored projects, ranging from best practices in computational thinking to technology implementation. She serves on the editorial boards of Information & Management and the ACM Journal of Data and Information Quality and her research has been published in leading academic journals.
 Alain Pinsonneault is a James McGill professor and the Imasco chair of information systems in the Desautels faculty of management at McGill University. He is also a fellow of the Royal Society of Canada, fellow of the Association for Information Systems, and a member of the Ordre National du Québec. His current research interests include the organisational and individual impacts of information technology, user adaptation, social networks, business model in the digital economy, e-health, e-integration, strategic alignment of IT, and the business value of IT. His research has appeared in numerous journals.
Alain Pinsonneault is a James McGill professor and the Imasco chair of information systems in the Desautels faculty of management at McGill University. He is also a fellow of the Royal Society of Canada, fellow of the Association for Information Systems, and a member of the Ordre National du Québec. His current research interests include the organisational and individual impacts of information technology, user adaptation, social networks, business model in the digital economy, e-health, e-integration, strategic alignment of IT, and the business value of IT. His research has appeared in numerous journals.