by Joan Costa-i-Font and Mario Gyori

Worldwide obesity has nearly tripled since 1975, with 39 percent of adults overweight in 2016 and 13 percent obese. Today the overweight population exceeds the underweight population worldwide, which remains true even for the majority of middle-income countries. Obesity is associated with several chronic diseases such as high blood pressure, high cholesterol, type II diabetes, cancer, heart disease and arthritis. Estimates from industrialised countries show that health care costs for obese people are 36 percent higher, and medication costs 77 percent higher, than for people in a normal weight range. High levels of obesity therefore pose a substantial risk to both the wellbeing of affected individuals and the sustainability of public health systems.
However, there are important differences in the prevalence of obesity and its socioeconomic determinants across the world. One important difference lies in the cross-country differential in obesity and overweightness associated with cultural habits and preferences. Some of these differences relate to gender, in that overweight and obesity rates are higher among women than men. According to the WHO, 15.1 percent of women worldwide were obese in 2016, compared to only 11.1 percent of all men. One of the parts of the world where these gender differences are particularly pronounced is the Middle East.
Middle Eastern Paradox
The ‘Middle Eastern gender health inequality paradox’ is that overweightness and obesity among women in the MENA region occurs with much higher frequency than among men. Figure 1 shows that the region has one of the highest rates of female obesity prevalence on earth.
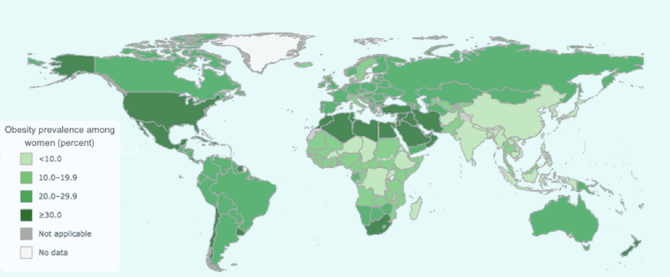
Table 1 sheds further light on gender differences with regards to obesity and illustrates that men in the Middle East are much less affected by the obesity epidemic than women. Only 15.7 percent of the men in the region are affected by obesity, which is close to the worldwide average for men. On the other hand, 26 percent of all women are obese – almost twice the world average. In several countries female obesity rates even surpass 40 percent, while male obesity rates in the same countries remain far below (only amounting to 22.7 percent in Egypt, 28.2 percent in Jordan and 30.8 percent in Saudi Arabia). Furthermore, in the region’s poorer and more politically unstable countries like Yemen and Iraq, female obesity rates far surpass those for male obesity. The table also illustrates that this phenomenon is not new – obesity differentials between men and women have been remarkably constant over the last three decades.
Table 1: Gender Obesity Gaps in the MENA region in 1990 and 2016
| 1990 | 2016 | |||||
|---|---|---|---|---|---|---|
| Male obesity | Female obesity | Percentage point difference female-male | Male obesity | Female obesity | Percentage point difference female-male | |
| Egypt | 9.7% | 25.2% | 15.5 | 22.7% | 41.1% | 18.4 |
| Saudi Arabia | 14.4% | 28.5% | 14.1 | 30.8% | 42.3% | 11.5 |
| Tunisia | 6.9% | 19.6% | 12.7 | 19.1% | 34.3% | 15.2 |
| Yemen | 2.9% | 8.2% | 5.3 | 12.0% | 22.0% | 10.0 |
| MENA region | 5.8% | 14.3% | 8.5 | 15.7% | 26.0% | 10.3 |
| World | 5.0% | 8.6% | 3.6 | 11.1% | 15.1% | 4.0 |
Our Middle East Centre research project attempts to understand this gender difference in health based on econometric analyses and experimental evidence. Societies in Middle Eastern countries have been increasingly exposed to western habits, lifestyle, culture and populations, with some regions experiencing greater levels of influence – or resistance – compared to others. Industrialisation and globalisation have contributed in this direction. As a result, a number of health outcomes, such as obesity, overweightness, or smoking, have been affected. In particular, our aim is to identify any gaps that might exist across countries and investigate whether/how such gaps depend on a number of determinants including but not limited to social norms, socioeconomic factors, lifestyle and environmental characteristics, and food prices.
Obesity and Gender
Recent health economics research examining cross country body mass index gaps between European countries has been able to pin down lifestyle, socio-economic and socio-environmental factors as determinants of obesity. This research has identified the importance of social environment in explaining the BMI gap, while other arguably relevant predictors show no statistical effect. We hypothesise that peer, partner, or social pressures, differences in attitudes, or social norms might be responsible for any gaps that might be present, and could thus have some significant explanatory power. Costa-i-Font et al. attempt to explain the BMI gap between Spain and Italy using counterfactual quantile regression analysis. Their results suggest the existence of a BMI gap in females, especially the young, a fact mainly attributable to behavioural differences. Their findings highlight the importance of eating habits and education, as being the primary predictors explaining the BMI gap between men and women. Micklesfield et al. find similar results in a study on South African women and underline in particular that black women may face cultural and socio-economic barriers to physical activity.
Conclusion
Gender differences in obesity and overweight are reflective of differences in preferences and culture. However, we know little about the underlying determinants of such differences. Our research for the LSE Middle East Centre attempts to gain new insights on the determinants of the ‘gender obesity gap’ in the MENA region.
*This blogpost introduces the LSE Academic Collaboration project Explaining the Middle Eastern Health Inequality Paradox run in collaboration with Zayed University and the United Arab Emirates University, examining the gender gap in Middle Eastern obesity rates and the reasons behind it. Joan Costa-i-Font is Principal Investigator and Mario Gyori is a researcher in the LSE Research Team.
Joan Costa-i-Font is an Associate Professor (Reader) at the LSE’s European Institute and the Department of Health Policy. He is also a CESifo (Munich) and IZA (Bonn) Research Fellow. Joan is also Principal Investigator on the LSE Middle East Centre project, ‘Explaining the Middle Eastern Health Inequality Paradox‘.
is an Associate Professor (Reader) at the LSE’s European Institute and the Department of Health Policy. He is also a CESifo (Munich) and IZA (Bonn) Research Fellow. Joan is also Principal Investigator on the LSE Middle East Centre project, ‘Explaining the Middle Eastern Health Inequality Paradox‘.
Mario Gyori is a Research Associate at the UNDP’s International Policy Centre for Inclusive Growth in Brasilia, Brazil. He is also a researcher on the LSE Middle East Centre project, ‘Explaining the Middle Eastern Health Inequality Paradox‘.
is a Research Associate at the UNDP’s International Policy Centre for Inclusive Growth in Brasilia, Brazil. He is also a researcher on the LSE Middle East Centre project, ‘Explaining the Middle Eastern Health Inequality Paradox‘.





Modern drugs and inhaler has allowed people an average and healthy life.
Treatment method can as well as take care of some other accompanying indicators, as an illustration eczema or decreased
immunity. Foods which contain vitamin E and C are viewed inn lowering the inflammatory response inside the lungs of folks that experience asthma.
Obserge the party all together by capturing the party on camera not with the
quantity of photos you take. s act without Gellar oor his manager being able to see them before filming.
Products are adced and subtracted every once in awhile while they become available.