 Why is there more tobacco control policy than alcohol control policy in the UK? Paul Cairney examines their post-war histories to demonstrate ‘paradigm’ change in tobacco, but not alcohol, policy. Tobacco control policy is more advanced in key areas, including a ban on advertising and promotion, high taxes to discourage consumption, unequivocal health education and warning labels on products. He argues that a focus on ‘the evidence’ can only partially explain policy change, since the gap between evidence and a proportionate tobacco policy response was 20-30 years. The ‘evidence matters’ when policymakers accept it and have the motive and opportunity to act on it.
Why is there more tobacco control policy than alcohol control policy in the UK? Paul Cairney examines their post-war histories to demonstrate ‘paradigm’ change in tobacco, but not alcohol, policy. Tobacco control policy is more advanced in key areas, including a ban on advertising and promotion, high taxes to discourage consumption, unequivocal health education and warning labels on products. He argues that a focus on ‘the evidence’ can only partially explain policy change, since the gap between evidence and a proportionate tobacco policy response was 20-30 years. The ‘evidence matters’ when policymakers accept it and have the motive and opportunity to act on it.
‘The evidence does not speak for itself’ is a truism in policy studies. Evidence based policymaking (EBPM) is about power: to decide what counts as evidence; to ignore or pay attention to particular studies; to link the evidence of a policy problem to a particular solution; and, to ensure that policymakers have the motive and opportunity to turn a solution into policy. Indeed, an attempt to portray EBPM as a technical or scientific process is often an attempt to exercise power: to rule some evidence in and most evidence out; and, to use particular forms of evidence to justify political action.
A comparison of tobacco and alcohol policy in the UK demonstrates this point well. Both examples show us the importance of a ‘battle of ideas’ between public health groups and private companies. In tobacco, it looks like that battle has been won (although issues such as e-cigarettes still arise). The scientific evidence, linking both smoking and second-hand smoking to major illness and premature death, has been accepted within government. The evidence is also stated unequivocally, allowing public health groups to argue that there is no safe level of smoking and that a series of measures should be introduced to minimise smoking in the population as a whole. Policy is ‘comprehensive’, involving a range of measures – including a ban on tobacco advertising and promotion, a ban on smoking in public places, high taxes to discourage smoking, unequivocal health education, graphic warning labels on products, and smoking cessation services – designed to reinforce the effect of each other. Policy change has been ‘paradigmatic’, involving a complete shift in the way that governments have understood, and sought to address, the policy problem. Smoking was once a normal or even glamorous activity. Now, it has been ‘denormalised’ by government. To give one sense of that shift, consider that many governments allowed adverts, which implied that smoking was healthy, in the post-war era. Only 50-60 years later, it is portrayed as unhealthy and reckless (particularly when around children).
In alcohol, the battle rages on. There is no equivalent to the acceptance of unequivocal evidence within government. Instead, the debate focuses increasingly on the idea that there is a safe (and perhaps even beneficial) level of alcohol consumption. This makes it more difficult to advocate blanket controls (which annoy ‘sensible drinkers’) rather than specific measures (to deal with ‘problem drinkers’). So, alcohol control is relatively ‘weak’ on measures such as advertising and promotion, taxation and health education (although note that the Scottish Government has some responsibility, and it recently legislated to introduce a minimum unit price for alcohol). The industry spends £200million per year on advertising and £600-800million on marketing; while the main avenue for health education is an organisation funded £6million per year by the industry. Drinking is still a normal part of life and government policy does not challenge its normality to the same extent as in tobacco.
While this may look like a straightforward case of EBPM – alcohol control is weaker because the evidence is weaker – the history of tobacco control suggests otherwise. If we examine the post-war history of tobacco, we see that the link between the initial production of the scientific evidence (which we now take for granted) and a ‘comprehensive’ government response was 20-30 years. The evidence is now well established and often taken for granted, but it was ignored by government (or, at least, not acted upon) for a long time. Comprehensive tobacco control may seem inevitable now but, until at least the 1980s, it looked just as unlikely as alcohol control.
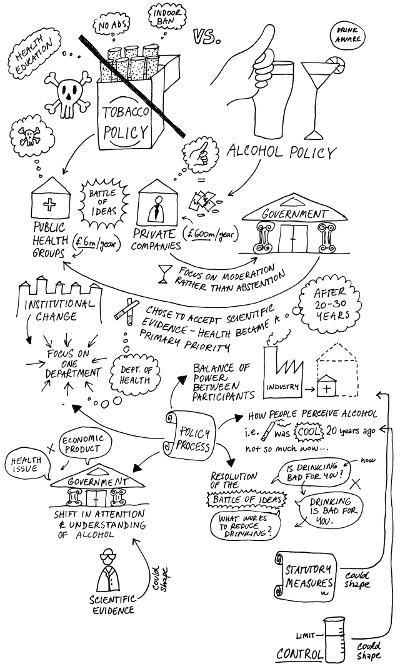
This is not just an interesting example of EBPM for the academics. It is also a key comparison for public health groups and the alcohol industry, as shown in Figure 1 below. Both groups are looking to learn from the experience of tobacco policy change; to guide their strategies on alcohol.
Figure 1 – Tobacco vs Alcohol policy
A history of UK tobacco control, informed by the literature on public policy theory, may not provide either side with a blueprint for action, but it does show them the evidence-to-policy context in which they operate. We can break the policy process down into five key factors to consider what would have to happen for alcohol control to mimic tobacco control:
- Institutional change. Institutions are the rules and norms that guide policymaking behaviour. Each government department may have its own rules on information gathering (what sources do they seek and which groups do they consult?). A key change in tobacco is that the Department of Health eventually became the focal point for tobacco action – a change that influenced how the tobacco problem was understood and addressed in government. In alcohol, a range of departments may be involved, including the Home Office (antisocial behaviour, licensing), DCMS (licensing, tourism, leisure), Transport (drink driving) and Treasury and trade departments (these differences between tobacco and alcohol can also be found at the EU level).
- A shift in attention to, and understanding of, alcohol. Tobacco is now perceived within government to be a public health problem to be solved (rather than an economic product to be encouraged). The need for greater tobacco control also rose up the government agenda at key stages in policy development. The government’s perception of alcohol is more mixed. It may recognise the health element, but be unsure about a general public health approach compared to a focus on problem drinkers (or other groups, such as young drinkers) and anti-social behaviour. It may promote ‘sensible’ drinking rather than abstention. It may also view alcohol as a product with economic value, central to the ‘night time economy’ and linked to measures to encourage the tourism and leisure industry. In contrast, the Treasury finally gave up this economic image in tobacco when it took joint responsibility for policy on health inequalities (and its review in 2002 found that smoking is the primary source of inequality).
- A shift in the balance of power between participants. In tobacco, the post-war period has been marked by a profound shift within government, from the privileged consultation to the exclusion of the tobacco industry within government (a shift accelerated by the release of internal tobacco company documents). Public health groups, once at the periphery of policymaking when directed by economic departments, are now at the centre of policy driven by the health department. In alcohol, the industry still plays a significant part of government strategies (and there is not an alcohol equivalent of the ‘smoking gun’, although groups are now trying to find it). Further, it is responsible for the implementation of voluntary agreements on advertising and health promotion, which give it a reason to be consulted routinely by government (voluntary agreements are generally criticised by public health groups). This relationship with groups is central to the type of evidence a government gathers, its interpretation of the evidence, and the advice it receives.
- A shift in the socioeconomic context. In tobacco, we witnessed a steady post-war fall in smoking (from 65-82% men/ 41% women in 1948 to 21%/ 19% in 2011); the tax revenue from tobacco (from 15% of government revenue in 1950 to 3-4% now) and public opposition to control (which also tends to fall further after controls have been introduced). All three factors produced an environment more conducive to policy change. In alcohol, the economic benefit of alcohol consumption (or, the importance of the tax revenue to the Treasury), the number of drinkers, and opposition to alcohol control may still be a factor (although recent polls highlight a fine balance of support/ opposition for a minimum unit price of alcohol).
- The resolution of the battle of ideas. The scientific evidence linking smoking and passive smoking to ill health is now ‘set in stone’ in government. The evidence is not questioned in the way that it once was. Instead, governments have shifted their attention to the evidence on ‘what works’ to reduce smoking (see for example the ‘Tobacco Control Scale’ topped by the UK). This took some time: the scientific evidence on smoking developed from the 1950s but major tobacco control did not emerge until the 1980s; the evidence on passive smoking emerged from the 1980s but a ‘smoking ban’ was introduced in the mid-2000s. In alcohol, there is still debate about the safe/ beneficial level of consumption and the extent to which governments should encourage harm reduction rather than abstention. There may also be a considerable gap between the acceptance of new evidence in government and a proportionate government response – particularly since the industry plays a role in interpretation in a way long rejected in tobacco.
The tobacco experience suggests that changes in these factors are mutually reinforcing; major policy change is the result of the complex interplay between all of these processes For example, an increased acceptance of the unequivocal alcohol-is-harmful scientific evidence would help shift the way that governments ‘frame’ or understand the alcohol policy problem. The framing of alcohol as a public health problem would allow the health department to take the policy lead and consult primarily with public health groups. Alcohol control and alcohol use may also go hand in hand: a decrease in drinking rates reduces the barriers to alcohol control; more alcohol control means fewer drinkers (or less drinking). The replacement of voluntary alcohols with statutory measures would reduce the routine involvement of the industry in government.
It is tempting to think that policy change is more likely under Labour and less likely under the Conservatives – and there is some evidence to back up this argument. For example, the Labour Government in 1997 made a much stronger commitment to tobacco control than its Conservative predecessor. Some tobacco (plain packaging) and alcohol (MUP) controls also seem to have stalled after the election of a Conservative-led government. However, a focus on the post-war history also shows us that these long term processes develop during the terms of both parties, and policy change is not reversed after a change in government. In other words, tobacco and alcohol control has a cumulative effect beyond the terms of parties.
Overall, the post-war experience of tobacco control provides some positive and negative lessons for public health groups seeking to strengthen the regulation of alcohol (and vice versa for the industry and critics of the ‘nanny state’). On the one hand, it shows us that policy environments which once seemed resistant to public health solutions at one point in time have become conducive in another. The obstacles to contemporary alcohol control resemble those in tobacco before policy began to change profoundly from the 1980s. On the other hand, major policy change, of the level we have witnessed in tobacco, took several decades. The evidence plays a key part in that process, but ‘comprehensive’ policy change is neither quick nor inevitable.
This article is based on a longer paper, How and Why are Public Health Ideas Accepted by Policymakers? Comparing Tobacco and Alcohol Control.
Note: This article gives the views of the author, and not the position of the British Politics and Policy blog, nor of the London School of Economics. Please read our comments policy before posting.
About the author
Paul Cairney is Professor of Politics and Public Policy at the University of Stirling. He does comparative public policy, including the study of single issues across the globe (tobacco control), multiple issues (including health, education and local government) in Scottish and UK politics, and the comparison of policy theories. He tweets @cairneypaul and his blog is at http://paulcairney.blogspot.co.uk/.





{Link removed. Drop previous submission.}
Michael J. McFadden says:
Your comment is awaiting moderation.
July 10, 2013 at 5:13 am
I find it interesting that the entire and EXTREMELY important role of denormalization through the creation of fear of secondary smoke is being ignored in this article (unless I missed it along the way somehow…) It was that fear that turned the public indifference about smoking into a public tolerance of widespread discrimination in terms of taxation, bans, and even hiring and housing. It also largely ignores the “Save The Children” propaganda weapon that has been so skillfully used by Antismokers both in terms of secondary exposure and in terms of creating and playing “the addiction card” for smoking… despite the fact that both the 1964 and 1979 Surgeon General’s Reports came out quite clearly against any blanket declaration of smoking as being addictive according to normal English and scientific language usage.
The Children and addiction elements *will* be brought in against alcohol, and will be brought in by the same folks who brought you The Great American Antismoking Crusade (as Don Oakley so aptly titled it in his 1999 “Slow Burn…”). After all, don’t you know that 93% of all drinkers began drinking as children (i.e. under 21)? Drinking is *clearly* a “pediatric disease” in the same sense as smoking, and just look at the billions upon billions of dollars of expenditure that have been poured into the latter.
Secondhand alcohol? Might seem funny at first glance, but read my analysis in the BMJ’s Rapid Responses by Googling:
“michael j. mcfadden” vaughn database
and choosing “Secondary Smoke, Alcohol, and Deaths.” I wrote that eight years ago and have offered it up in hundreds of internet discussions since then, and aside from poking fun at an idea that could be even more exaggerated than secondhand smoke, no one has challenged it on any basic grounds. Just wait till the day when you order a Dom Perignon with your dinner at a fancy restaurant and are told that you have to take it back behind the dumpsters in the alley to chug a few quick gulps if you want.
The nonsmoking drinkers out there threw the smokers to the wolves. If the forces of Free Choice don’t prevail, they’ll soon find themselves on the set of the “Alien” movie: Be Afraid. Be VERY Afraid.
Michael J. McFadden
Author of “Dissecting Antismokers’ Brains”
Right, Professor. And what has this vast expenditure of time and money produced of any significance?
A smoking ban in some enclosed places.
And upon what is the paltry result based?
Two massive lies:
1. That private property is public property.
2. That second hand smoke is dangerous.
Brilliant.
That’s Mr Dr Professor.
You might like this too: http://dickpuddlecote.blogspot.co.uk/2013/07/an-lse-guide-on-how-to-denormalise.html?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed:+DickPuddlecote+(Dick+Puddlecote)
Whatever…..
Also note that the full paper was co-authored with Professor Donley Studlar (University of Strathclyde). I’d also like to thank my agent and you, the reader.
The drawing was done by @zascreativebag – see here http://paulcairney.blogspot.co.uk/2013/07/how-do-people-read-your-research.html
The new Tobacco Prohibition
I would like to take the time to tell the entire community about a falsehood so big that everyone who believes in freedom should be appauled.
This falsehood is so big it resonates from historical fact forward to this day. This falsehood is so big billions of dollars have been spent to make it believable to those of us who dont take the time to look up the facts.
We all remember reading about alcohol prohibition,but did you know there was also tobacco prohibition going on before alcohol became such a target of the last nanny staters.
Our great grandparents lived thru prohibition and the great depression,they also lived thru tobacco prohibition.
Heres a time line starting in 1900,dont be surprised to see the same thing playing out today nearly 100 years later.
1901: REGULATION: Strong anti-cigarette activity in 43 of the 45 states. “Only Wyoming and Louisiana had paid no attention to the cigarette controversy, while the other forty-three states either already had anti-cigarette laws on the books or were considering new or tougher anti-cigarette laws, or were the scenes of heavy anti- cigarette activity” (Dillow, 1981:10).
1904: New York: A judge sends a woman is sent to jail for 30 days for smoking in front of her children.
1904: New York City. A woman is arrested for smoking a cigarette in an automobile. “You can’t do that on Fifth Avenue,” the arresting officer says.
1907: Business owners are refusing to hire smokers. On August 8, the New York Times writes: “Business … is doing what all the anti-cigarette specialists could not do.”
1917: SMOKEFREE: Tobacco control laws have fallen, including smoking bans in numerous cities, and the states of Arkansas, Iowa, Idaho and Tennessee.
1937: hitler institutes laws against smoking.This one you can google.
Now onto the falsehood……
We have been told for years by smoke free advocates that second hand smoke is the cause of everything from johnnys ear ache to cousin ED’S lung cancer. But wheres the proof!!!
Remember they claim 50,000 deaths a year yet,there are no bodys not even mass graves of the dead to second hand smoke.We await the names of these victims.
A simple stroll down historys road say 10 years or so and we start to get at the truth……
A federal Judge by the name of osteen got a case dropped in his lap in North Carolina,the case was that of EPA’S study on second hand smoke/environmental tobacco smoke.The judge an anti-tobbaco judge by reputation spent 4 years going thru the study and interviewing scientists at EPA and came to the conclusion :
JUNK SCIENCE
”EPA’s 1992 conclusions are not supported by reliable scientific evidence. The report has been largely discredited and, in 1998, was legally vacated by a federal judge.Before its 1992 report, EPA had always used epidemiology’s gold standard CI of 95 percent to measure statistical significance. But because the U.S. studies chosen[cherry picked] for the report were not statistically significant within a 95 percent CI, for the first time in its history EPA changed the rules and used a 90 percent CI, which doubled the chance of being wrong.
This allowed it to report a statistically significant 19 percent increase [a 1.19rr] of lung cancer cases in the nonsmoking spouses of smokers over those cases found in nonsmoking spouses of nonsmokers. Even though the RR was only 1.19–an amount far short of what is normally required to demonstrate correlation or causality–the agency concluded this was proof SHS increased the risk of U.S. nonsmokers developing lung cancer by 19 percent.”
The EPA fought to have Osteen’s decision overturned on technical grounds, ignoring the multitude of facts in the decision. They succeeded in 2002 on the narrowest of technicalities. The fourth circuit court of appeals ruled that because the report was not an official policy document Osteen’s court did not have jurisdiction. In their appeal the EPA did not answer a single criticism in the 92 page report, nor challenge a single fact put forth by Judge Osteen. Not one.
Although the anti-smoker movement was already established, this report was used, and continues to be used, to bolster their claim that SHS is a killer.
http://knol.google.com/k/secon… #
So here we find that second hand smoke was made a political scapegoat by EPA.Lets not forget how EPA has reworked the global warming studys just this last summer. Where its top scientists paper was rebuked because it didnt carry the EPA’S stand that global warming was real.
The political shenanigans surrounding SHS/ETS go deep not only with the government and its health agencies but also to the big pharmaceutical companies and non-profit orginizations aka ACS,ALA,AHA and a meriad of others. All lobbying for smoking bans and their weapon of choise Propaganda paid for by big pharma and tax dollars. Studys made to order that second hand smoke is deadly. Take a memory note here too,over 250 studys on shs/ets have found it safe.
Yet a simple look at the chemistry shows us that its:
About 90% of secondary smoke is composed of water vapor and ordinary air with a minor amount of carbon dioxide. The volume of water vapor of second hand smoke becomes even larger as it quickly disperses into the air,depending upon the humidity factors within a set location indoors or outdoors. Exhaled smoke from a smoker will provide 20% more water vapor to the smoke as it exists the smokers mouth.
4 % is carbon monoxide.
6 % is those supposed 4,000 chemicals to be found in tobacco smoke. Unfortunatley for the smoke free advocates these supposed chemicals are more theorized than actually found.What is found is so small to even call them threats to humans is beyond belief.Nanograms,picograms and femptograms……
(1989 Report of the Surgeon General p. 80).
Now, how odd that when we search the smoke free activists sites not one of them mentions that water vapor and air are the main components of second hand smoke. Is this just a fluke or an outright omission to further their political healthscare against the general public.
The last informative tid bit I have for you is what does OSHA have to say about all this secondhand smoke stuff.
Here is where it gets interesting,it seems John Banzhaf, founder and president of Action on Smoking and Health (ASH) decided to sue OSHA to make a rule on shs/ets not that OSHA didnt want to play ball with him,its just that the scientific facts didnt back up a rule to start with.
Now for a rule to happen Osha has to send out for comments for a period of time and boy did the comments fly in, over 40,000 of them….Osha has whats called PEL’S and limits for an 8 hour period of exposure to chemicals in indoor environments…[epa is in charge of outdoor air]some smoke free groups have tried to use 30 minute air samples using epa monitoring to create a air borne healthscare.
The actual standard to use is OSHA’S
The EPA standard is to be used for OUTSIDE ambient air quality and it is the average over a period of 3 years.
The proper standard to compare to is the OSHA standard for indoor air quality for respirable particulate (not otherwise specified) for nuisance dusts and smoke. That standard is 5000 ug/m3 on a time-weighted average (8 hours a day, 5 days a week) and is intended to be protective of health over an average working life of 30 years!
This is where second hand smoke really becomes a joke,remember its nearly 90% water vapor and air…..now lets get to the facts of toxicology and dose makes the poison:
According to independent Public and Health Policy Research group, Littlewood & Fennel of Austin, Tx, on the subject of secondhand smoke……..
They did the figures for what it takes to meet all of OSHA’S minimum PEL’S on shs/ets…….Did it ever set the debate on fire.
They concluded that:
All this is in a small sealed room 9×20 and must occur in ONE HOUR.
For Benzo[a]pyrene, 222,000 cigarettes
“For Acetone, 118,000 cigarettes
“Toluene would require 50,000 packs of simultaneously smoldering cigarettes.
Acetaldehyde or Hydrazine, more than 14,000 smokers would need to light up.
“For Hydroquinone, “only” 1250 cigarettes
For arsenic 2 million 500,000 smokers at one time
The same number of cigarettes required for the other so called chemicals in shs/ets will have the same outcomes.
So,OSHA finally makes a statement on shs/ets :
Field studies of environmental tobacco smoke indicate that under normal conditions, the components in tobacco smoke are diluted below existing Permissible Exposure Levels (PELS.) as referenced in the Air Contaminant Standard (29 CFR 1910.1000)…It would be very rare to find a workplace with so much smoking that any individual PEL would be exceeded.” -Letter From Greg Watchman, Acting Sec’y, OSHA, To Leroy J Pletten, PHD, July 8, 1997
WHAT! DILUTED BELOW PERMISSABLE LEVELS
By the way ASH dropped their lawsuit because OSHA was going to make a rule and that rule would have been weak and been the law of the land,meaning no smoking bans would ever have been enacted anywhere,simply because an open window or a ventilation system would have covered the rule.
Let me also tell you that the relative risk for shs/ets by the SG report of 2006 was a 1.19 ”EPA study is whats used to call it a carcinogen”……milks is a 2.43 and that glass of chlorinated water your about to drink is a 1.25 yet these things aren’t determined to be a carcinogen….The gold standard in epidemiology is a 3.0….Now had the SURGEON GENERAL included 2 other shs/ets studys the relative risk for disease from shs/ets would have been nearer a.60-.70 meaning it would have a protective effect against ever getting disease.
But,what each of us has is years and years of exposure and the knowledge that our kids all grew up around shs and generations of others,yet we are here alive not dead from a lousy 30 minute exposure to shs as stanton glantz tries to claim…..thats another story and its just as crazy as all the rest of smokefree’s claim about shs/ets.
Oh! have you heard the one about ”laugh” thirdhand smoke or third hand drinking.
Like I said their claims border beyond that of any reasonable persons commomsence.
The next time you see a healthscare claim
consider the source.Especially if it comes from a government or non profit agency!