In March 2010, President Obama signed the Patient Protection and Affordable Care Act, which marked the most comprehensive reform of the American health care system since the Johnson Administration. This federal legislation makes the American states key political stakeholders for achieving major goals of the reform, one of which is to make health insurance coverage more inclusive and equal. Focusing on the state-level picture, Ling Zhu and Jennifer H. Clark examine how partisan politics produce far-reaching distributional consequences in health care. They show that inequality in health insurance coverage persists at the state level, especially in conservative states with diverse populations.
In March 2010, President Obama signed the Patient Protection and Affordable Care Act, which marked the most comprehensive reform of the American health care system since the Johnson Administration. This federal legislation makes the American states key political stakeholders for achieving major goals of the reform, one of which is to make health insurance coverage more inclusive and equal. Focusing on the state-level picture, Ling Zhu and Jennifer H. Clark examine how partisan politics produce far-reaching distributional consequences in health care. They show that inequality in health insurance coverage persists at the state level, especially in conservative states with diverse populations.
In the American health care system, individuals can obtain health insurance coverage from different sources. According to the Kaiser Family Foundation’s recent report, more than half of the non-elderly Americans have employment-sponsored health insurance coverage. About six percent of the non-elderly Americans are covered by privately -purchased insurance plans. Medicaid, State Children’s Health Insurance Program (SCHIP), and other public programs cover about 20 percent of the non-elderly Americans. Federally funded Medicare covers elderly Americans who have retired from the workforce. As a result, both the labor-market and the generosity of public programs affect how health insurance is distributed across different income levels.
Using a Gini-Coefficient measure of inequality, we compare the level of inequality in pre-redistribution and post-transfer health insurance coverage across the fifty states. For example, Figure 1 illustrates how we assess inequality in pre-redistribution (i.e. privately provided) insurance coverage in Texas in 2007. Figure 1 shows, private health insurance coverage varies substantially across family income levels, with individuals from lower income groups having much lower coverage rates. The corresponding Gini-coefficient measure of inequality captures how the distribution of insurance coverage is skewed toward high-income groups, with a value close to 1 indicating a high level of inequality, and a value close to 0 indicating a low level of inequality. As shown in Figure 1, Texas had a quite high-level of inequality in private health insurance coverage in 2007.
Figure 1 – Distribution of Private Health Insurance Coverage across Nine Family Income Levels in Texas 2007
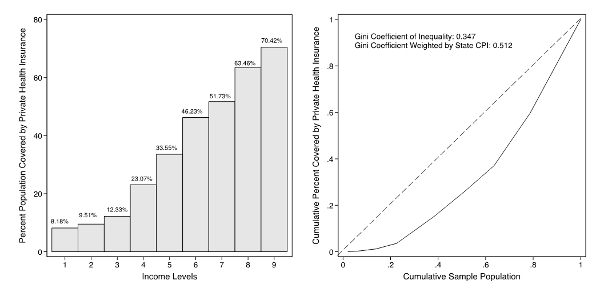
Note: Data are based on the U.S. Census Bureau 2008 Current Population Surveys
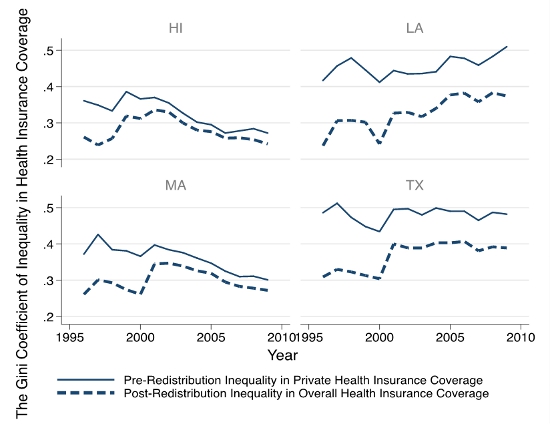
Figure 2 further shows how both pre- and post-redistribution inequality in health insurance coverage changed from 1996 to 2009 in Massachusetts, Hawaii, Louisiana, and Texas. Massachusetts and Hawaii, as two leading states in regulating employment-based health insurance, have relatively low levels of inequality in private health insurance coverage. These two states also have generous public coverage through Medicaid and SCHIP; therefore, they have low levels of inequality in overall health insurance coverage. A few southern states, such as Louisiana and Texas, have high levels of both private and overall health insurance coverage. Both Massachusetts and Hawaii show small “gaps” between the two inequality measures, indicating that in these two states, market-based insurance coverage is relatively inclusive, and public health insurance programs equalizes the distribution of health care.
Figure 2- Inequality in Pre- and Post-Redistribution Health Insurance Coverage in Louisiana, Hawaii, Massachusetts, and Texas, 1996-2009.
Partisan Politics, Ethnic Diversity and Health Care Inequality
What explains the varying-level of inequality in health insurance coverage? Our research shows that state-level partisan politics have far-reaching distribution consequences in the health care domain, especially in states with diverse populations.
Partisan balance of state legislatures makes a difference. Our analysis of data on the fifty states in a 17-year time period suggests that there is a negative association between the proportion of Democratic legislators in state legislatures and inequality in both private and overall health insurance coverage. States with a large share of Democratic legislators, especially those with a Democratic supermajority, are more likely to have generous public health insurance programs; therefore, these states are able to include more low-income individuals in their public health insurance programs (e.g. Medicaid and SCHIP). We also find that private insurance markets are more regulated in Blue states than those in Red states, particularly regarding regulations and tax-incentives for encouraging small-business employers to provide insurance coverage to their employees.
Racial diversity of state population is a key context of understanding health inequality. In the recent two decades, many American states have experienced increasing racial/ethnic diversity of their populations. This important demographic change is largely driven by the rapid growth of the native-born Hispanic population and immigration. We discover that health insurance coverage is more unequal in states with heterogeneous populations than in states with homogeneous populations. Our research also finds that Democratic-controlled state legislatures reduce health care inequality more substantially in states with a high level of racial diversity than in states with a low level of racial diversity, while inequality in health insurance coverage has been persistently high in Republican-controlled states with diverse populations.
States’ Critical Role in Reducing Health Care Inequality
At the state level, the provision of health care is largely a function of political institutions, labor-market bias, and racial diversity. How well the uneven distribution of health care coverage is addressed upon complete implementation of the Affordable Care Act is largely dependent on the 50 state governments. Given our finding of a central role of partisanship in the provision of health care insurance coverage, it is conceivable the specific kinds of reforms offered at the state level are critical to reducing disparities in health insurance coverage. The state’s role in implementing key provisions of the Affordable Care Act, such as the expansion of Medicaid and the creation and maintenance of state health insurance exchanges, will provide a unique opportunity to examine how different types of policies advanced by Democrats and Republicans influence health care outcomes and how this relationship differs in accordance with racial and ethnic diversity of the state.
This article is based on the paper, “Rights without Access: The Political Context of Inequality in Health Care Coverage in the U.S. States” in State Politics and Policy Quarterly.
Image credit: Chris Potter, stockmonkeys.com (CC-BY-2.0)
Please read our comments policy before commenting.
Note: This article gives the views of the author, and not the position of USApp– American Politics and Policy, nor of the London School of Economics.
Shortened URL for this post: http://bit.ly/1bAAHy0
_________________________________
Ling Zhu – University of Houston
Ling Zhu is an Assistant Professor of Political Science at the University of Houston. Her research interests include public management, health disparities, social equity in healthcare access, and the implementation of public health policies at the state and local level.
Jennifer Hayes Clark- University of Houston
Jennifer Hayes Clark is an Associate Professor of Political Science and a Research Associate at the Center for Public Policy at the University of Houston. Her primary areas of research interest include American political institutions, public policy, and quantitative research methodology.