Sanna Read, Raphael Wittenberg, and Nicholas Mays summarise research carried out by a team from the Policy Innovation and Evaluation Research Unit (a collaboration between LSE’s Care Policy and Evaluation Centre and the London School of Hygiene and Tropical Medicine) examining whether people think social care should be funded by the state, or whether service users should continue to contribute to the cost. They find that three out of four want the state to contribute more but the user to continue to pay at least for some of the social care costs.
There is widespread agreement that the system of financing social care in England needs reform, but no agreement on how it should be reformed. There have been many proposals for reform over the last 20 years, but none has been implemented. Unlike healthcare, social care is not free at point of use: access to publicly funded social care is subject to an assessment of financial means (income and savings) as well as care needs. A key issue is how much service users should be expected to pay toward the costs of their care and how this should vary with their income and savings.
While debate on how best to fund social care continues, information about public attitudes to funding is limited. For example, should the housing wealth of care home residents continue to be taken into account in the means test for care? Currently, residents who own their home are generally ineligible for public funding. Should service users who have savings be expected to use them to fund their care? Service users who have more than £23,250 currently have to meet the full costs of their care. And should users be required to contribute to their care costs from their incomes? At present, they have to contribute all their income above prescribed thresholds.
New ways of studying a complex topic – use of vignettes and profiles
In December 2018, we carried out an online survey of public preferences on social care in old age with the help of Kantar to address these questions. The study included 3000 people living in England between the ages of 18 and 75. It was informed by the findings of a set of focus groups that explored views about paying for care.
A major challenge is that social care in old age is a complex topic on which the majority of the public has little knowledge or personal experience. To overcome this problem, the questionnaire included a short introduction to social care in England, i.e. what social care involves, who receives social care, and how it is paid for. Respondents were then presented with four vignettes describing the life circumstances of fictitious older people – named either Grace or Alan – facing home care or residential care costs with different levels of financial resources. They were asked to indicate their preferences regarding the contributions the state and Grace or Alan should make towards the costs of their social care. The options varied between care paid fully by the state, fully by the service user, or shared between the two, and at varying levels of Grace or Alan’s savings, income and housing wealth. We also asked a general question on the best way to pay for care, with the response categories ranging from ‘State should pay for all’ to ‘Everyone should make their own arrangements’.
Key findings – share the cost!
Nearly 60% of people in England think that costs of social care in old age, such as help at home and staying in a care home, should be shared between the state and the individual (Figure 1). Currently, about half of all people receiving adult social care pay for at least part of their care costs. The majority like to continue to share the cost. However, compared with the current arrangements, they believe that the public share should be greater and come into play earlier rather than only when people have run down their financial resources.
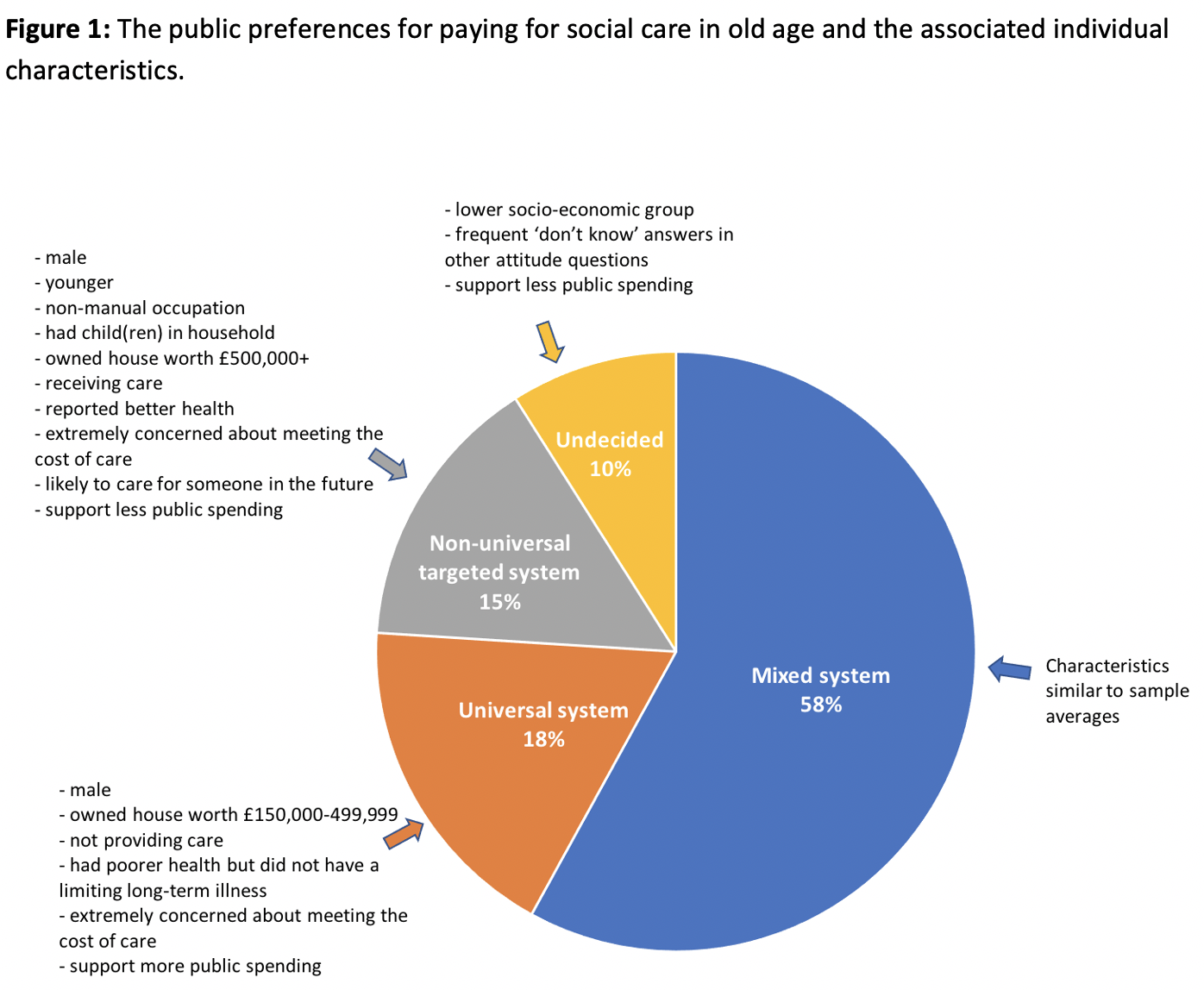
A smaller proportion, 18% of survey respondents, prefer a universal system under which costs of care are met by the state even for service users with substantial resources. This would be similar to the current healthcare system (NHS). Only 15% of respondents prefer a non-universal targeted system under which costs of care are met by service users unless they have insufficient resources. This would be broadly similar to the current social care system in England. Two smaller groups (each about 5% of respondents) are undecided in their preferences for paying for care with some or frequent ‘I don’t know’ answers.
According to our survey, most people want the state to contribute more than it currently does under England’s existing funding system. Many also support the idea that the state should pay for basic care which people could then top up. There is only limited support for social care in old age to be arranged similarly to healthcare (NHS), free at the point of use. Even fewer favour a system similar to the current social care funding rules. The majority support a reformed system where social care is highly subsidised by the state, but where people who use services contribute in all cases to the costs of their care.
Public attitudes on paying for social care vary with people’s demographic and socio-economic characteristics. The main group – those proposing that costs should be shared between the state and the individual – have similar characteristics to the general population aged 18 to 75, suggesting that a majority of general public would support this approach.
Those proposing a universal system of state-funded care and those preferring that service users meet the full costs of their care until they have exhausted their resources interestingly shared some characteristics: they are more often men and home-owners than those advocating that costs should be shared, and they have a very high level of concern about the costs of care. On the other hand, these two groups are different in other respects: those favouring that all costs be met by service users have more financial means, better self-rated health, more caring responsibilities and prefer less public spending compared to those who prefer a universal system of paying for care. These findings challenge the idea that those who are wealthier and who have experience of care and its costs would support free care funded by the state.
Do the results reflect the methods used or the public’s sense of realism?
These findings are in line with some recent studies showing that a relatively large proportion (up to half of the sample) propose shared responsibility between the state and the individual for paying for care. However, our study, unlike some others, suggests that only a small proportion prefer universal, state-funded care in old age, like the NHS. This difference in findings may be due to the method we used. The public often have little knowledge of how social care funding is arranged and how much care recipients need to contribute to the costs. Our method of using vignettes provides a realistic description of care needs, care costs and levels of service users’ financial resources. Detailed information on the current situation may influence people’s views. The information provided in the vignettes may increase support for the view that those benefitting from care and having financial resources might be expected to take some responsibility for paying for their own care, most often in partnership with the state.
The results may also reflect public reaction to the ongoing debate on social care funding. Successive governments have repeatedly claimed to be prioritising social care funding reform but failed to make any changes. This experience may have reduced public expectations of the likelihood of any further effective collective responsibility for meeting the costs of social care. More generally, such attitudes would be consistent with the impact of more than a decade of financial austerity and the longer-term consequences of neoliberal economics for the implied social contract between the state and the public.
____________________
Note: The above draws on independent research commissioned and funded by the National Institute for Health Research (NIHR) Policy Research Programme through its core support to the Policy Innovation Research Unit (Project No: 102/0001). The views expressed are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
 Sanna Read is Assistant Professorial Research Fellow in the Care Policy and Evaluation Centre at the LSE.
Sanna Read is Assistant Professorial Research Fellow in the Care Policy and Evaluation Centre at the LSE.
 Raphael Wittenberg is Deputy Director and Associate Professorial Research Fellow in the Care Policy and Evaluation Centre at the LSE.
Raphael Wittenberg is Deputy Director and Associate Professorial Research Fellow in the Care Policy and Evaluation Centre at the LSE.
 Nicholas Mays is Professor of Health Policy at the London School of Hygiene and Tropical Medicine.
Nicholas Mays is Professor of Health Policy at the London School of Hygiene and Tropical Medicine.




When doing these surveys are people asked their perception on nursing care and social care, their opinions on the fee differences between self funders and what local authorities pay. So much emphasis is said on social care but a large percentage of self funders have complex issues such as stroke but classed as social needs