The impact of the COVID-19 pandemic on people of different ethnicities in England has invited a lot of attention, but poorer outcomes of some groups have still not been fully explained. Lucinda Platt explores the reasons why it is important to recognise the complex background factors involved that may influence both infection and severity, and how they are interlinked.
The impact of the COVID-19 pandemic on people of different ethnicities in England has invited a lot of attention, but poorer outcomes of some groups have still not been fully explained. Lucinda Platt explores the reasons why it is important to recognise the complex background factors involved that may influence both infection and severity, and how they are interlinked.
The very strong age-related gradient of the coronavirus has resulted in the largest numbers of deaths among older (predominantly White British) people. As of 29 January 2021, there had been over 105,000 COVID-19-related deaths in England, of which 90% were aged 65 or over and, of those with recorded ethnicity, 88% were White, slightly more than the White population share. Yet given that most of the UK’s ethnic minority groups have a younger age profile, the expectation would be for them to make up an even lower percentage of COVID-related deaths.
In fact, once the fatality rates are adjusted for age, the death rate for minority groups has been disproportionately higher, albeit with some variation by specific group. While most of the analysis has been carried out on individuals in private households, deaths in care homes were also higher for Black and Asian minority groups. Numerous candidates for these differences in risks have been proposed—and to some extent tested.
The link between deprivation and facing enhanced risks from COVID-19 has been clearly articulated. Such deprivation has been evaluated in terms of area deprivation, socio-economic position, census-based measures of deprivation, and overcrowding. Since ethnic minorities are more likely to be living in poor families and deprived areas, a counting for these levels of deprivation has mediated some, though not all, of the excess risks faced by specific minority ethnic groups. Given how particular health conditions increase the severity of the impact of COVID-19, analyses have also adjusted for relevant health conditions and hospitalisations, which again explain an additional share of the disparities but still leave unexplained gaps. A further disparity relates to rates of survival among those admitted to hospital, which showed ethnic group differences that were particularly severe for Bangladeshis. Again, adjusting for pre-existing health conditions (and for other factors) reduces but does not close this gap.
It is important to recognise, however, that both the presence of relevant health conditions and their severity may be linked to prior patterns of persistent disadvantage and discrimination, complicating the relationship between prior health, deprivation, and COVID-19 mortality. In addition, those health conditions that are linked to high risks of mortality from COVID-19 may also be more or less severe and more or less well managed across ethnic groups. For example, Mathur and colleagues found differences in the management of diabetes by ethnic group. This can mean that such health conditions have a greater impact on the lives and overall health of some more than others; and simply controlling for underlying conditions may not capture these relevant differences. It is striking, in relation to this point, that Office for National Statistics (ONS) analysis showed that disability – i.e the limiting consequences of chronic conditions – was associated with an elevated risk of COVID-19 mortality, even after controlling for a whole suite of relevant health conditions and hospitalisations.
It seems plausible, therefore, that the extent to which serious health conditions are or are not well-treated and therefore are or are not experienced as disabling may explain some of the differences in COVID-19 mortality across ethnic groups. This is relevant given that we know that there are striking differences across ethnic groups in the prevalence of disability among older working age adults from research using a comparable definition to that of the ONS research of longstanding, activity-limiting ill-health. The same study also showed that the experience of disability across ethnic groups differed in terms of the extent to which multiple morbidities were experienced concurrently.
To provide a more current perspective on this issue, Table 1 below describes the rates both of longstanding health problems (a broader measure than the ONS disability definition) and the experience of multiple morbidities (more than one named health condition) for men and women in the age band 45–59 across ethnic groups in the period 2016–2019. As it shows, Bangladeshi men and women and Pakistani women of this age are more likely to have a longstanding health problem and multi-morbidities than the White British, while those from the Other White and Black African ethnic groups in this age range are rather less likely to—also consistent with earlier research.

Source: Platt, 2021, Table 1. Analysis of Labour Force Survey, 2016 Q1 to 2019 Q4 (weighted).
As well as the individual directly affected, disabilities affect the households in which they live. For example, the presence of a disabled person may mean that another member of the household has caring responsibilities and is thus more constrained in terms of their ability to participate in the workforce. If the disabled person contracts COVID-19, the carers are then themselves vulnerable. So, the household context is relevant to how we understand transmission and COVID-19 risks. Given that there is substantial variation in household composition across ethnic groups, with larger average sizes and greater risks of overcrowding among certain groups, particularly Bangladeshis, and that there are increased risks of transmission the more people in the household, individual risks and the household risks are linked. To illustrate, while fewer than one in four White British working-age households contain someone with a health condition that is relevant for risks of COVID-19 severity, this rises to nearly one in three Pakistani and Bangladeshi households. So far, the ways in which analysis has attempted to take into account deprivation, housing and household circumstances, and elevated risks of specific health conditions does not sufficiently acknowledge how mutually implicated all these factors are.
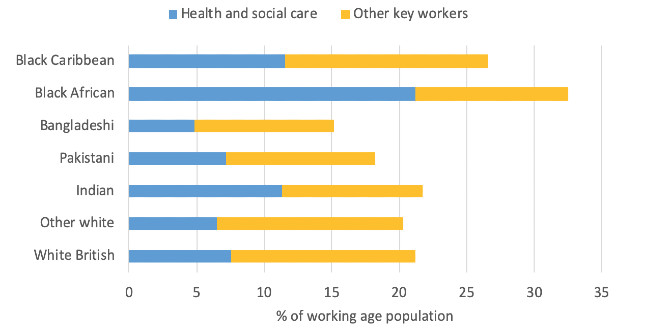
In addition, the fact that ethnic minorities may be disproportionately employed in roles that carry elevated risk of exposure to COVID-19 has been identified as a possible contributing factor to their elevated mortality risk. Certain occupations require workers to frequently come into close contact with others. This enhances their risk of contracting the virus, particularly given that, in many of these roles, the relative intimacy means there is an elevated risk of receiving a high viral load. Analysis bears this out, with studies showing substantial differences in risk across particular occupations, such as care workers, home carers, nurses, and nursing auxiliaries. It is notable that many, if not all, of the occupations identified as having significantly higher COVID-19 mortality risks are those in which specific ethnic minority groups are over-represented. This includes care workers, among whom Black African men and women are particularly highly represented, as well as security guards, bus drivers, retail workers, and those working in hospitality and catering. The role of occupational exposure as a contributory factor in death rates is also suggested by the markedly lower average age at death for Black Africans (mid-60s) compared to other ethnic groups, which have an average age at death of over 70 and in the high 70s for the white majority. This difference in average age at death is across the Black African group as a whole, not just those in high-risk occupations, but it indicates that a far higher share who have died from COVID-19 were in work.
Once again, such occupational risks cannot be considered independently of the household context. Risks of exposure and transmission do not just affect the individual but also those they live with. Households with workers in exposed occupations are therefore likely to have increased chances of intra-household transmission. Consistent with this, here is a growing body of evidence that larger household sizes and/or multigenerational households are associated with greater infection and mortality risks. Ethnic minorities tend to live in larger households, to have higher rates of multigenerational households, and to be more at risk of living in overcrowded households and households without a garden. These factors all increase the risks of intra-household transmission and higher viral load when there is infection within the household. Both these occupational and housing patterns need, however, to be understood in relation to deprivation or exclusion from which they stem, rather than being considered as independent cultural characteristics. Such recognition may take us further in understanding the deep-seated routes of the current inequalities in COVID-19 mortality risks and their implications for policy.
___________________
Note: The above is an edited extract from the author’s published work in the LSE Public Policy Review (available open access here).
Lucinda Platt is Professor of Social Policy and Sociology in the Department of Social Policy at the London School of Economics and Political Science. Her most recent book is Understanding Inequalities: Stratification and Difference, Polity, 2019, new edition.
Photo by hosein zanbori on Unsplash.